Pregnancy & Sciatica
Sciatica During Pregnancy: Safe Treatments (2026)
Sciatica during pregnancy affects 1 in 3 women. Discover safe treatments, exercises, and proven relief strategies for every trimester in 2026.
Sciatica during pregnancy is one of the most common yet under-discussed discomforts expectant mothers face. Affecting up to one in three pregnant women, this shooting nerve pain can range from a mild annoyance to a debilitating condition. The good news: safe, effective treatments exist for every trimester — no medication required.
By Dr. Rachel Nguyen, DPT — Last updated: March 2026
Table of Contents
- What Is Sciatica During Pregnancy?
- Why Pregnancy Triggers Sciatica
- Recognising the Symptoms
- Safe Treatments by Trimester
- Best Exercises for Pregnancy Sciatica
- Sleep Positions That Reduce Sciatic Pain
- Recommended Products for Pregnancy Sciatica Relief
- When to See Your Doctor
- Sciatica After Delivery: What to Expect
- Frequently Asked Questions
- Sources and Methodology
- Medical Disclaimer
What Is Sciatica During Pregnancy?
Sciatica refers to pain that radiates along the path of the sciatic nerve — the longest nerve in your body. This nerve runs from your lower back, through your hips and buttocks, and down each leg. During pregnancy, changes in your body can compress or irritate this nerve, producing symptoms that range from a dull ache to sharp, shooting pain.

It is important to understand that true sciatica — caused by compression of the sciatic nerve root at the spine — is actually less common in pregnancy than posterior pelvic pain, which mimics sciatica symptoms. Research published in the European Spine Journal suggests that while up to 80% of pregnant women experience some form of back pain, true lumbar radiculopathy (nerve root compression) occurs in roughly 1% of pregnancies. The more common culprit is piriformis syndrome or sacroiliac joint dysfunction, both of which produce sciatica-like symptoms.
Regardless of the precise cause, the pain is real, and the treatment approaches overlap significantly. Throughout this guide, we use "pregnancy sciatica" to encompass all forms of sciatic-type nerve pain during pregnancy.
Why Pregnancy Triggers Sciatica
Understanding what causes your pain helps you choose the right treatment. Several pregnancy-specific changes contribute to sciatic nerve irritation:
Weight Gain and Shifting Centre of Gravity
As your baby grows, your centre of gravity shifts forward. This causes an exaggerated lumbar curve (lordosis) that compresses the structures around the sciatic nerve roots. The average weight gain of 11 to 16 kilograms during pregnancy places significant additional load on the lumbar spine and pelvis.
Hormonal Changes
Your body produces increased levels of relaxin during pregnancy, a hormone that loosens ligaments in the pelvis to prepare for delivery. While essential for childbirth, this ligament laxity can destabilise the sacroiliac joints and allow subtle shifts that irritate the sciatic nerve.
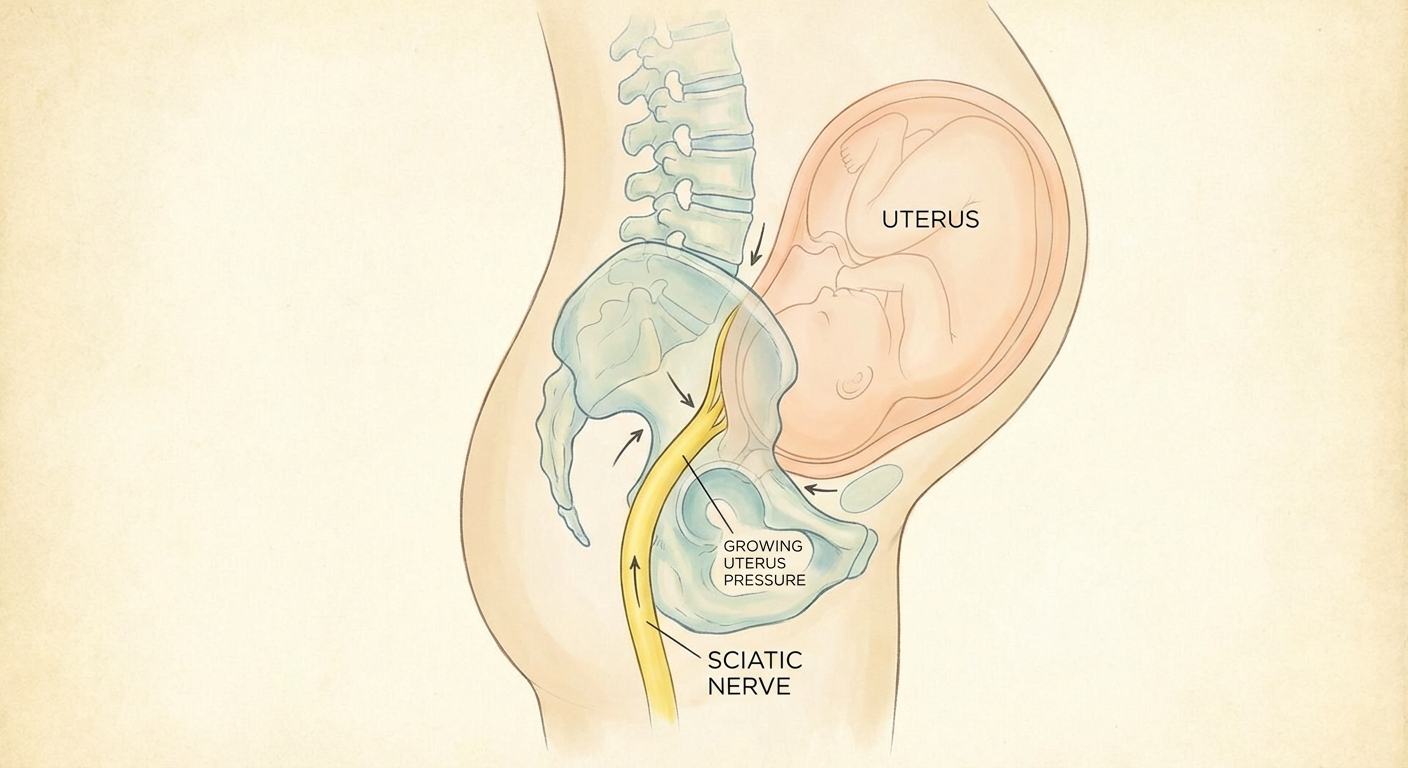
Baby's Position
In the third trimester particularly, the baby's head can rest directly on the sciatic nerve as they settle into the pelvis. This direct pressure is one reason why sciatica symptoms often intensify in the final weeks of pregnancy.
Fluid Retention
Increased blood volume and fluid retention during pregnancy can cause swelling around the nerve pathways, contributing to compression and irritation.
Pre-existing Disc Issues
If you had a herniated or bulging disc before pregnancy, the postural and hormonal changes of pregnancy can exacerbate existing nerve compression. Women with a history of lower back problems are at higher risk for pregnancy sciatica.
For a deeper understanding of how nerve compression works, our guide on what causes sciatica covers the full range of underlying mechanisms.
Recognising the Symptoms
Pregnancy sciatica typically presents as:
- Sharp or burning pain radiating from the lower back or buttock down one leg
- Numbness or tingling in the affected leg or foot
- Pain that worsens when sitting, standing for long periods, or climbing stairs
- Difficulty walking or a sensation that your leg might give way
- One-sided symptoms — sciatica almost always affects one side only

Sciatica vs. Normal Pregnancy Back Pain
Not all back pain during pregnancy is sciatica. Here is how to tell the difference:
Normal pregnancy back pain tends to be a generalised ache across the lower back, often related to muscle fatigue and postural strain. It typically affects both sides equally and does not radiate below the knee.
Pregnancy sciatica produces a distinct radiating pattern — pain that travels from the buttock or lower back down the back of the thigh and potentially into the calf or foot. It is usually one-sided and may include tingling, numbness, or a pins-and-needles sensation.
If your symptoms include leg weakness, loss of bladder or bowel control, or sudden severe pain, seek medical attention immediately. These may indicate cauda equina syndrome, a rare but serious condition requiring urgent treatment.
Safe Treatments by Trimester
The cornerstone of treating sciatica during pregnancy is conservative, non-pharmaceutical management. Most healthcare providers recommend a combination of physical approaches tailored to your stage of pregnancy.
First Trimester (Weeks 1–12)
During the first trimester, sciatica is relatively uncommon since weight gain and postural changes are minimal. If symptoms do appear, they likely relate to pre-existing conditions aggravated by hormonal changes.
Safe approaches include:
- Gentle stretching, particularly the piriformis stretch and seated spinal twist
- Walking for 20 to 30 minutes daily on flat surfaces
- Applying a warm (not hot) compress to the lower back for 15 to 20 minutes
- Maintaining good posture, especially if you work at a desk
- Prenatal yoga classes designed for the first trimester
Second Trimester (Weeks 13–26)
This is when many women first notice sciatica symptoms as the baby grows and your body adapts. Treatment options expand during this stage:
Safe approaches include:
- Prenatal physical therapy with a pelvic health specialist
- Swimming or water aerobics — buoyancy relieves spinal compression
- Pregnancy support belts to redistribute weight
- Side-lying position during rest (left side preferred for circulation)
- Foam rolling the piriformis and gluteal muscles (with guidance)
- Prenatal massage from a certified therapist

Third Trimester (Weeks 27–40)
The third trimester is the peak period for pregnancy sciatica. The baby is at their heaviest, postural changes are most pronounced, and the pelvis is loosening in preparation for delivery.
Safe approaches include:
- All second-trimester approaches, modified for comfort
- Pelvic tilts and cat-cow stretches to relieve lumbar pressure
- Ice packs on the piriformis area for acute flare-ups (10 to 15 minutes maximum)
- Hands-and-knees position to shift baby's weight off the nerve
- Acupuncture — evidence suggests it can be safe and effective in the third trimester
- Transcutaneous electrical nerve stimulation (TENS), with your provider's approval
Understanding the full range of sciatica treatment options can help you and your provider choose the safest approach for your stage of pregnancy.
What to Avoid During Pregnancy
Certain common sciatica treatments are not safe during pregnancy:
- NSAIDs (ibuprofen, naproxen) — avoid especially after 20 weeks due to risks of premature closure of the ductus arteriosus
- Oral steroids — generally avoided due to potential effects on fetal development
- Spinal injections — epidural steroid injections are typically deferred until after delivery
- Deep tissue massage directly on the abdomen or certain acupressure points
- Inversion therapy or any inverted positions after the first trimester
If you experience sciatica alongside other musculoskeletal pain, you may find our sciatica stretches and exercises guide helpful for additional safe movement options.
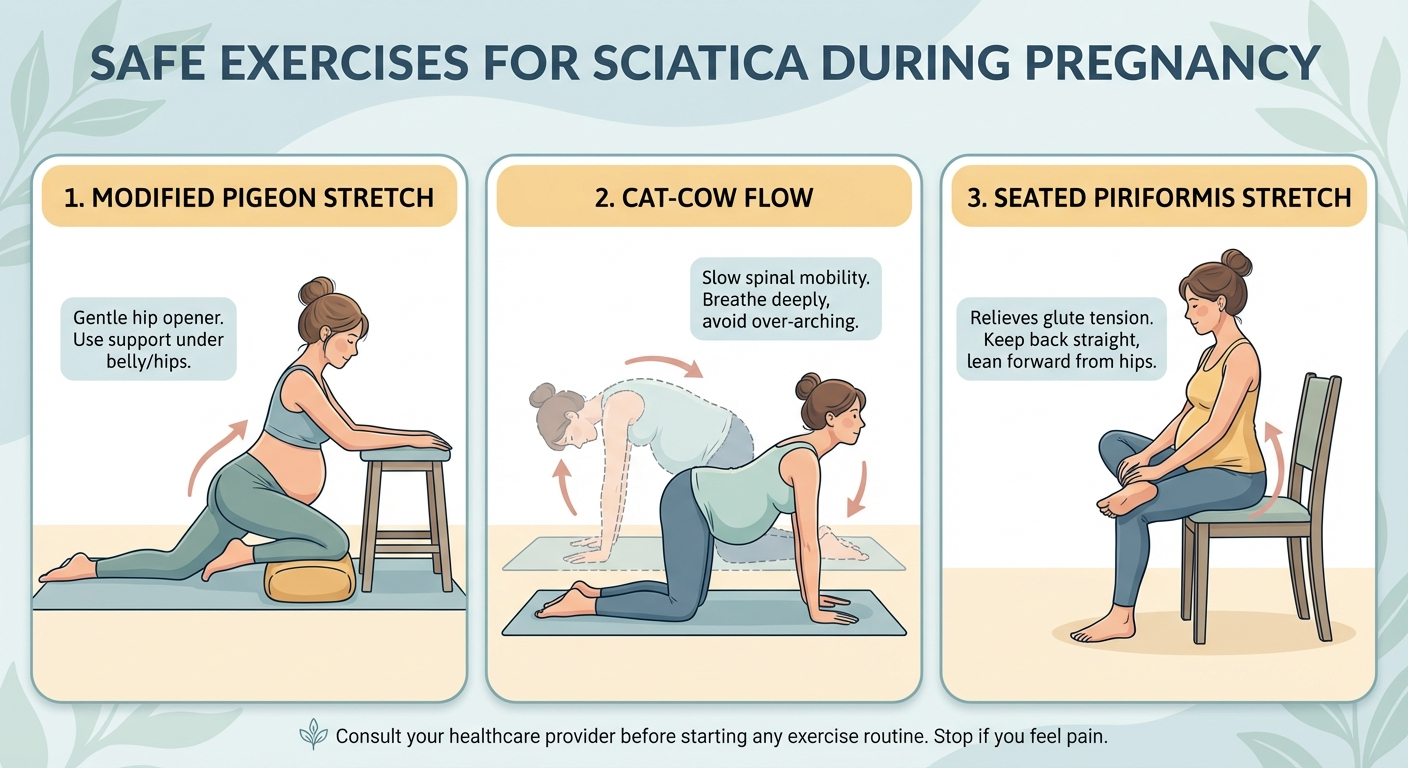
Best Exercises for Pregnancy Sciatica
Movement is medicine for pregnancy sciatica. The following exercises are generally safe across all trimesters, though you should always clear new exercises with your prenatal care provider.
1. Seated Piriformis Stretch
The piriformis muscle sits deep in the buttock and can compress the sciatic nerve when tight. This stretch targets it directly.
- Sit on a chair with both feet flat on the floor
- Cross the ankle of your affected leg over the opposite knee
- Keeping your back straight, lean forward gently until you feel a stretch in the buttock
- Hold for 20 to 30 seconds, repeat 3 times on each side
2. Cat-Cow Stretch
This classic prenatal exercise relieves lumbar pressure and improves spinal mobility.
- Start on all fours with hands under shoulders and knees under hips
- Inhale as you drop your belly toward the floor, lifting your head and tailbone (cow)
- Exhale as you round your back toward the ceiling, tucking your chin and tailbone (cat)
- Repeat 10 times, moving slowly with your breath
3. Pelvic Tilts
Pelvic tilts strengthen the core muscles that support your lower back and can reduce nerve compression.
- Stand with your back against a wall, feet shoulder-width apart
- Flatten your lower back against the wall by gently tilting your pelvis forward
- Hold for 5 seconds, then release
- Repeat 10 to 15 times
4. Glute Bridge (Modified)
Strengthening the glutes helps stabilise the pelvis and reduce sciatic nerve irritation.
- Lie on your back with knees bent and feet flat on the floor (avoid lying flat on your back after 20 weeks — use a wedge under your right hip)
- Squeeze your glutes and lift your hips toward the ceiling
- Hold for 5 seconds at the top, then lower slowly
- Repeat 10 times
5. Child's Pose (Modified)
A restorative stretch that decompresses the lower spine.
- Kneel on the floor with knees wide apart to accommodate your belly
- Sit back toward your heels and extend your arms forward on the floor
- Rest your forehead on the floor or a pillow
- Hold for 30 seconds to 1 minute, breathing deeply
6. Standing Hip Flexor Stretch
Tight hip flexors contribute to the exaggerated lumbar curve that triggers sciatica.
- Stand in a staggered stance with one foot forward
- Tuck your pelvis under and shift your weight forward until you feel a stretch at the front of your back hip
- Hold for 20 to 30 seconds, repeat on both sides
Sleep Positions That Reduce Sciatic Pain
Sleep disturbance is one of the most frustrating aspects of pregnancy sciatica. Finding the right position can mean the difference between rest and misery.
The Side-Lying Position
Sleep on your side — ideally the side opposite to your pain — with a pillow between your knees. This keeps your pelvis neutral and prevents the top leg from pulling your spine out of alignment.
The Pillow Support System
For maximum relief, use a combination of pillows:
- Between the knees — a firm pillow to maintain hip alignment
- Under the belly — a small wedge or folded towel to support the weight of your uterus
- Behind the back — a body pillow to prevent rolling onto your back during the night

Positions to Avoid
- Flat on your back — after 20 weeks, this can compress the vena cava and reduce blood flow. It also increases lumbar lordosis and sciatic nerve pressure.
- Stomach sleeping — obviously impractical as pregnancy progresses, and places strain on the lower back even in early pregnancy.
Recommended Products for Pregnancy Sciatica Relief
The following products can complement your exercise and treatment routine. Each has been selected based on features relevant to pregnancy sciatica relief.
| Product | Best For | Price Range | Rating |
|---|---|---|---|
| Boppy Side Sleeper Pillow | Sleep support & hip alignment | $30–$45 | ⭐⭐⭐⭐⭐ |
| Babymoov Dream Belt | Nighttime belly support | $35–$50 | ⭐⭐⭐⭐½ |
| OPTP PRO-ROLLER (Soft) | Piriformis & glute release | $25–$40 | ⭐⭐⭐⭐ |
| Gabrialla Maternity Belt | Daytime walking support | $30–$55 | ⭐⭐⭐⭐½ |
| TheraPearl Hot/Cold Pack | Heat & cold therapy | $10–$20 | ⭐⭐⭐⭐⭐ |
Visual guide: Safe exercises and sleep positions for pregnancy sciatica relief
Boppy Side Sleeper Pregnancy Pillow
A compact side-sleeping pillow designed to support both belly and back simultaneously. The dual-panel design keeps your spine aligned without overheating.
Best for: Side-sleeping support and hip alignment
Key features: Machine washable cover, compact enough for shared beds, firm knee support panel
Babymoov Dream Belt Sleep Support
A lightweight maternity belt specifically designed for sleeping, this belt cradles your belly and reduces the pulling force on your lower back and sciatic nerve during the night.
Best for: Nighttime belly support without bulk
Key features: Adjustable elastic, memory foam pad, fits weeks 15 through 40
OPTP PRO-ROLLER Foam Roller (Soft Density)
A soft-density foam roller ideal for gentle piriformis and glute release during pregnancy. The softer density is important — standard firm rollers can be too aggressive on pregnancy-sensitised tissues.
Best for: Piriformis and glute myofascial release
Key features: Soft EVA foam, 36-inch length for stability, round profile
Gabrialla Maternity Support Belt (Medium Support)
A prenatal support belt that lifts the belly and redistributes weight away from the pelvis and lower back. The medium-support level provides meaningful relief without restricting movement.
Best for: Daytime walking and standing support
Key features: Breathable mesh, adjustable velcro, fits under clothing, available in multiple sizes
TheraPearl Reusable Hot/Cold Pack
A versatile therapy pack that can be used warm or cold for sciatic flare-ups. The pearl-based design conforms to your lower back and buttock area better than rigid gel packs.
Best for: Alternating heat and cold therapy for acute flare-ups
Key features: Microwave and freezer safe, flexible when frozen, reusable, non-toxic
If your sciatica pain extends to tailbone discomfort — which is common in later pregnancy — you may also benefit from a specialised coccyx cushion. The team at Coccyx Relief has a thorough guide to seated support options that work well during pregnancy.
When to See Your Doctor
While most pregnancy sciatica is manageable with conservative treatment, certain symptoms warrant prompt medical attention:
- Progressive leg weakness — difficulty lifting your foot or walking normally
- Loss of bladder or bowel control — this may indicate cauda equina syndrome, a medical emergency
- Severe, unrelenting pain that does not respond to any position changes or home treatment
- Numbness in the groin or inner thighs (saddle anaesthesia)
- Fever accompanying back pain — may indicate infection
- Pain that started after a fall or injury
Your obstetrician or midwife can refer you to a prenatal physiotherapist or pelvic health specialist for targeted treatment. In some cases, an MRI without contrast may be used to evaluate severe symptoms, though imaging is generally reserved for cases that do not respond to conservative management.
Sciatica After Delivery: What to Expect
The majority of women with pregnancy-related sciatica experience significant improvement within weeks of delivery. Here is a general timeline:
Immediately after birth: Many women notice reduced pain as soon as the baby is delivered, particularly if the baby's position was a primary cause of nerve compression.
Weeks 1 to 6 postpartum: Residual inflammation and ligament laxity mean some symptoms may persist. Your body is still producing relaxin, especially if you are breastfeeding. Gentle walking and pelvic floor exercises support recovery.
Weeks 6 to 12 postpartum: Most pregnancy-related sciatica has resolved by this point. If symptoms persist beyond 12 weeks postpartum, a postnatal physiotherapy assessment is recommended to rule out ongoing structural issues.
Persistent postpartum sciatica: In a small percentage of women, sciatica continues after delivery. This may indicate a pre-existing disc issue or pelvic joint dysfunction that requires targeted treatment. A pelvic health physiotherapist can provide assessment and a recovery plan.
Frequently Asked Questions
Is sciatica during pregnancy dangerous to my baby?
Sciatica during pregnancy is not dangerous to your baby. The nerve pain affects your musculoskeletal system, not the uterus or placenta. However, severe pain can limit mobility and affect your quality of life, so managing symptoms is important for your overall wellbeing during pregnancy.
When does pregnancy sciatica usually start?
Pregnancy-related sciatica most commonly develops during the second and third trimesters, typically between weeks 24 and 36. This coincides with the period of greatest weight gain, postural changes, and hormonal shifts that loosen pelvic ligaments. Some women experience symptoms as early as the first trimester, though this is less common.
Can I take pain medication for sciatica while pregnant?
Acetaminophen (paracetamol) is generally considered safe during pregnancy for short-term pain relief when used at recommended doses. NSAIDs like ibuprofen should be avoided, especially after 20 weeks. Always consult your obstetrician or midwife before taking any medication during pregnancy, as recommendations can change based on your specific situation and trimester.
Does sciatica go away after giving birth?
For most women, pregnancy-related sciatica resolves within a few weeks to months after delivery. Once the baby is born, pressure on the sciatic nerve decreases, hormonal levels normalise, and postural alignment gradually returns. Some women experience immediate relief after birth, while others find symptoms taper off over 6 to 12 weeks postpartum.
What sleeping position helps sciatica during pregnancy?
Sleeping on your side with a pillow between your knees is the most recommended position for pregnancy sciatica. This keeps your hips, pelvis, and spine aligned, reducing pressure on the sciatic nerve. A full-length body pillow or wedge pillow under your belly provides additional support. Sleeping on the opposite side from where you feel pain often provides the most relief.
Are prenatal massages safe for sciatica during pregnancy?
Prenatal massage from a certified prenatal massage therapist is generally safe and can provide significant sciatica relief during pregnancy. Therapists trained in prenatal techniques know which areas to avoid and use appropriate positioning. Avoid deep tissue massage directly over the lower back in the first trimester, and always inform your therapist about your sciatica symptoms and how far along you are.


Sources and Methodology
This article draws on peer-reviewed medical research and established clinical guidelines for managing musculoskeletal pain during pregnancy:
-
Katonis, P., et al. (2011). "Pregnancy-related low back pain." Hippokratia, 15(3), 205–210. This review examines the prevalence and mechanisms of low back pain during pregnancy, including sciatic-type symptoms and their differentiation from true radiculopathy.
-
Vleeming, A., et al. (2008). "European guidelines for the diagnosis and treatment of pelvic girdle pain." European Spine Journal, 17(6), 794–819. These guidelines provide evidence-based recommendations for diagnosis and conservative management of pelvic pain during pregnancy, including sacroiliac joint dysfunction.
-
Liddle, S.D., & Pennick, V. (2015). "Interventions for preventing and treating low-back and pelvic pain during pregnancy." Cochrane Database of Systematic Reviews, (9). This Cochrane review evaluates the evidence for exercise, manual therapy, and other interventions for pregnancy-related back and pelvic pain.
-
American College of Obstetricians and Gynecologists (ACOG). Committee Opinion on exercise during pregnancy and the postpartum period. These guidelines inform the exercise recommendations and safety parameters discussed throughout this article.
Our methodology prioritises conservative, evidence-supported treatments. Product recommendations are based on features relevant to the conditions discussed and are not a substitute for professional medical advice. Where evidence is limited, we use hedging language and recommend consulting your healthcare provider.
Medical Disclaimer
The information provided in this article is for educational purposes only and is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your obstetrician, midwife, or other qualified healthcare provider with any questions you may have regarding sciatica during pregnancy or any other medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website. If you experience sudden severe pain, leg weakness, or loss of bladder or bowel control, seek emergency medical attention immediately.
{
"@context": "https://schema.org",
"@type": "FAQPage",
"mainEntity": [
{
"@type": "Question",
"name": "Is sciatica during pregnancy dangerous to my baby?",
"acceptedAnswer": {
"@type": "Answer",
"text": "Sciatica during pregnancy is not dangerous to your baby. The nerve pain affects your musculoskeletal system, not the uterus or placenta. However, severe pain can limit mobility and affect your quality of life, so managing symptoms is important for your overall wellbeing during pregnancy."
}
},
{
"@type": "Question",
"name": "When does pregnancy sciatica usually start?",
"acceptedAnswer": {
"@type": "Answer",
"text": "Pregnancy-related sciatica most commonly develops during the second and third trimesters, typically between weeks 24 and 36. This coincides with the period of greatest weight gain, postural changes, and hormonal shifts that loosen pelvic ligaments. Some women experience symptoms as early as the first trimester, though this is less common."
}
},
{
"@type": "Question",
"name": "Can I take pain medication for sciatica while pregnant?",
"acceptedAnswer": {
"@type": "Answer",
"text": "Acetaminophen (paracetamol) is generally considered safe during pregnancy for short-term pain relief when used at recommended doses. NSAIDs like ibuprofen should be avoided, especially after 20 weeks. Always consult your obstetrician or midwife before taking any medication during pregnancy, as recommendations can change based on your specific situation and trimester."
}
},
{
"@type": "Question",
"name": "Does sciatica go away after giving birth?",
"acceptedAnswer": {
"@type": "Answer",
"text": "For most women, pregnancy-related sciatica resolves within a few weeks to months after delivery. Once the baby is born, pressure on the sciatic nerve decreases, hormonal levels normalise, and postural alignment gradually returns. Some women experience immediate relief after birth, while others find symptoms taper off over 6 to 12 weeks postpartum."
}
},
{
"@type": "Question",
"name": "What sleeping position helps sciatica during pregnancy?",
"acceptedAnswer": {
"@type": "Answer",
"text": "Sleeping on your side with a pillow between your knees is the most recommended position for pregnancy sciatica. This keeps your hips, pelvis, and spine aligned, reducing pressure on the sciatic nerve. A full-length body pillow or wedge pillow under your belly provides additional support. Sleeping on the opposite side from where you feel pain often provides the most relief."
}
},
{
"@type": "Question",
"name": "Are prenatal massages safe for sciatica during pregnancy?",
"acceptedAnswer": {
"@type": "Answer",
"text": "Prenatal massage from a certified prenatal massage therapist is generally safe and can provide significant sciatica relief during pregnancy. Therapists trained in prenatal techniques know which areas to avoid and use appropriate positioning. Avoid deep tissue massage directly over the lower back in the first trimester, and always inform your therapist about your sciatica symptoms and how far along you are."
}
}
]
}
{
"@context": "https://schema.org",
"@type": "Article",
"headline": "Sciatica During Pregnancy: Safe Treatments (2026)",
"description": "Sciatica during pregnancy affects 1 in 3 women. Discover safe treatments, exercises, and proven relief strategies for every trimester in 2026.",
"author": {
"@type": "Person",
"name": "Dr. Rachel Nguyen, DPT"
},
"publisher": {
"@type": "Organization",
"name": "SciaticaSpot",
"url": "https://sciaticaspot.com"
},
"datePublished": "2026-03-20",
"dateModified": "2026-03-20",
"mainEntityOfPage": {
"@type": "WebPage",
"@id": "https://sciaticaspot.com/sciatica-during-pregnancy"
},
"image": "https://sciaticaspot.com/images/sciatica-during-pregnancy-hero.jpg"
}