Sciatica Treatment
Sciatica Surgery: When Is It Actually Necessary? (2026)
When does sciatica require surgery? A spine specialist-reviewed guide to surgical thresholds, procedure types, recovery timelines, risks, and non-surgical alternatives.
If you have been battling sciatica pain for weeks or months, you have probably wondered at some point: will I need surgery? The honest answer from spine specialists is that surgery is necessary for only a small fraction of sciatica cases — but when it is genuinely needed, it can be genuinely transformative. This guide separates the facts from the fear, so you can make an informed decision about your treatment path.
By Dr. Michael Torres, Physiotherapist | Last updated: April 2026
Table of Contents
- What Is Sciatica, Exactly?
- The First-Line Treatment: Why Conservative Care Comes First
- Red Flags: When Sciatica Becomes a Surgical Emergency
- The Surgical Threshold: When Do Doctors Recommend Surgery?
- Types of Sciatica Surgery: What Each Procedure Involves
- Comparing Sciatica Surgery Types
- Recovery After Sciatica Surgery: What to Expect
- Risks and Complications of Sciatica Surgery
- Failed Back Surgery Syndrome: What It Is and How to Avoid It
- Alternatives to Surgery: What Else Works?
- Questions to Ask Your Surgeon Before Going Under the Knife
- Frequently Asked Questions
- Sources and Methodology
What Is Sciatica, Exactly?
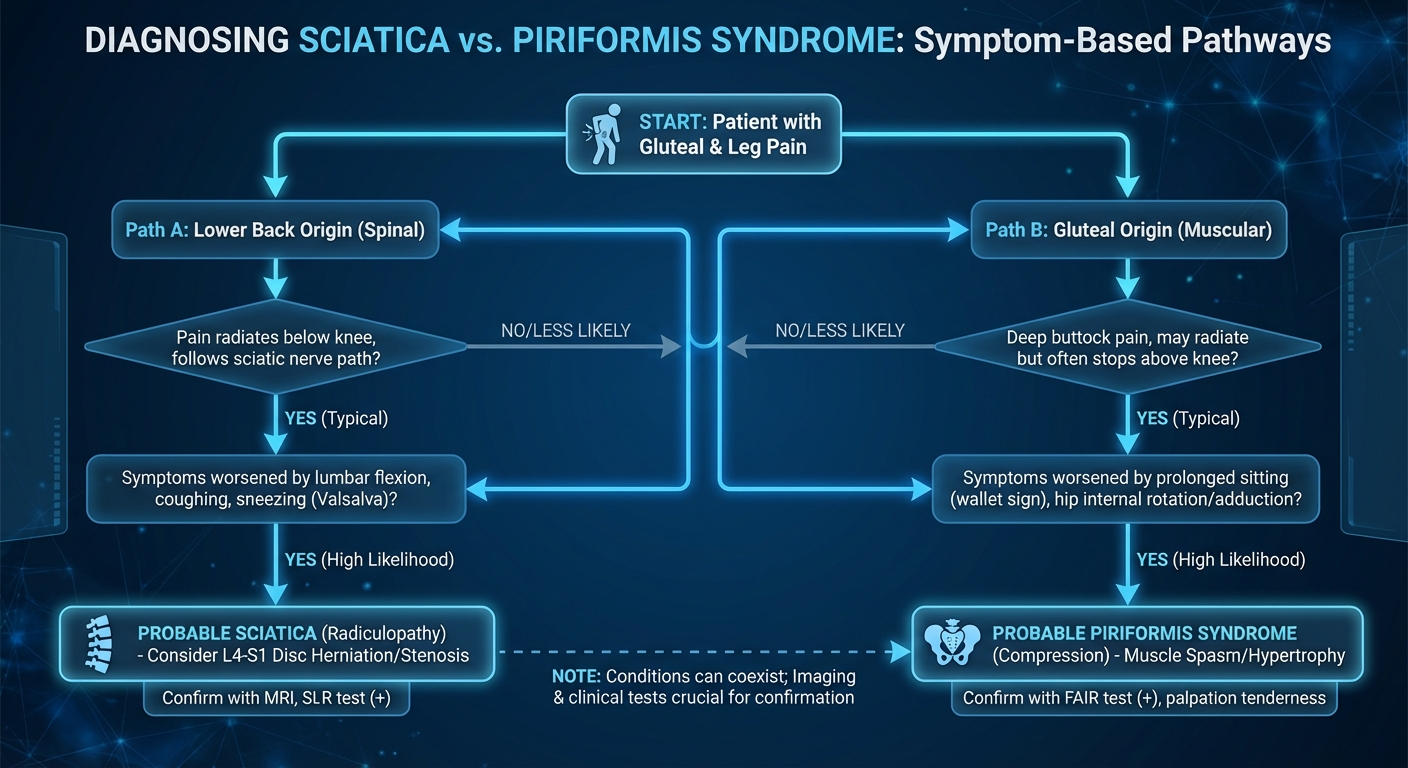
Sciatica is not a diagnosis — it is a symptom. It describes pain that radiates along the path of the sciatic nerve, which runs from your lower spine through your buttock and down the back of each leg. When something compresses or irritates this nerve, the result is a distinctive pattern of pain, tingling, numbness, or weakness that travels from the lower back into the leg, often extending past the knee and sometimes all the way to the foot.
The most common underlying causes include a herniated disc (responsible for roughly 90% of sciatica cases), spinal stenosis (narrowing of the spinal canal), piriformis syndrome (compression by a muscle in the buttock), or spondylolisthesis (one vertebra slipping over another). Less commonly, sciatica can result from tumors, infection, or trauma.
What makes sciatica distinctive from ordinary lower back pain is its nerve-specific pattern. Pain that radiates below the knee in a dermatomal distribution — following the path of a specific nerve root — is the hallmark clinical sign. Lower back pain without leg symptoms, by contrast, typically does not constitute sciatica and has a very different treatment approach.
Understanding this distinction matters enormously when deciding whether surgery is on the table. Surgery for sciatica works by removing whatever is pressing on the nerve. It does not treat generalized lower back pain, which is one reason why careful diagnosis before going to the operating room is so critical.
The First-Line Treatment: Why Conservative Care Comes First
Before anyone discusses surgery, the medical consensus — backed by decades of research — is that nearly all sciatica patients should begin with conservative (non-surgical) treatment. This is not a concession or a delay tactic. It reflects the fact that the vast majority of sciatica cases resolve on their own with time and appropriate care.
The research is consistent. A landmark 2000 study published in the New England Journal of Medicine found that for patients with sciatica caused by disc herniation, there was no significant difference in outcomes between those who underwent early surgery and those who pursued conservative care for an extended period. Both groups improved substantially over time.
Conservative treatment typically includes:
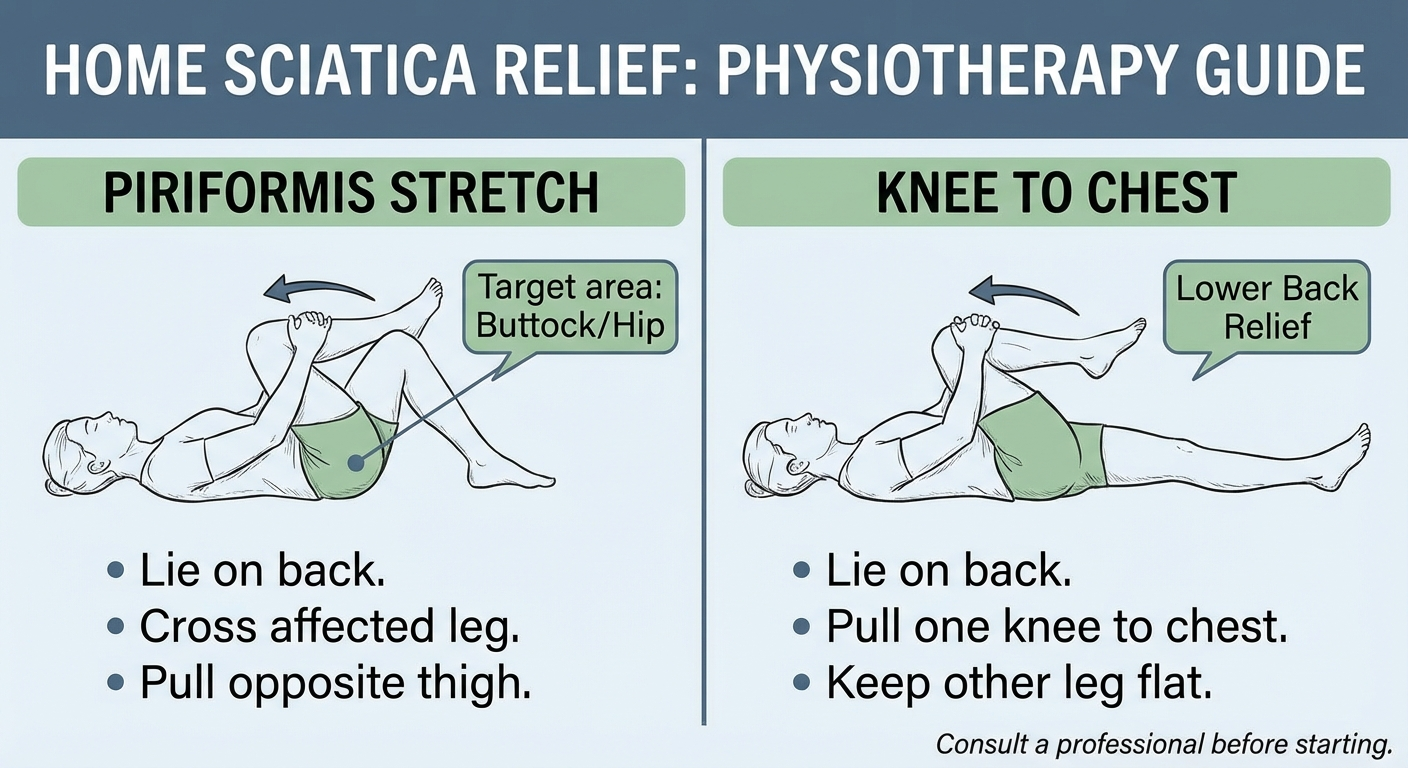
- Targeted physiotherapy — Specific exercises to reduce nerve compression, improve mobility, and stabilize the spine. Our sciatica exercises guide covers the most evidence-based movements.
- Medication — Non-steroidal anti-inflammatory drugs (NSAIDs) for pain and inflammation; neuropathic medications such as gabapentin for nerve-specific pain.
- Epidural steroid injections — A corticosteroid injected near the affected nerve root to reduce inflammation. Provides temporary but often meaningful relief that can allow you to participate more effectively in physiotherapy.
- Activity modification — Avoiding movements that aggravate the nerve while staying as active as tolerable.
- Heat and cold therapy — Used strategically during acute flare-ups to manage pain and muscle guarding.
The key principle is that conservative treatment gives your body the opportunity to heal itself. A herniated disc, for instance, shrinks over time through a process called resorption — the body's inflammatory response can gradually break down and absorb the extruded disc material, relieving pressure on the nerve naturally. Studies show that approximately 60-70% of herniated discs reduce in size or fully resolve without surgical intervention within six months.
Red Flags: When Sciatica Becomes a Surgical Emergency
While most sciatica is managed conservatively, a small subset of cases constitutes genuine medical emergencies requiring immediate surgical evaluation. These are the scenarios where waiting can result in permanent neurological damage — and in the most severe cases, life-threatening complications.
Cauda Equina Syndrome
This is the single most urgent indication for emergency spine surgery. Cauda equina syndrome (CES) occurs when the nerve roots at the very bottom of the spinal cord become severely compressed, disrupting bladder, bowel, and sexual function. The hallmark symptoms include:
- Saddle anesthesia — Numbness in the inner thighs, groin, buttocks, and perineum (the area that would contact a saddle)
- Loss of bladder or bowel control — Either urinary retention (inability to urinate) or fecal incontinence
- Severe or progressive leg weakness — Often affecting both legs
- Recent onset of sexual dysfunction
CES is a surgical emergency. The spinal cord itself ends around the L1-L2 level, below which the canal contains only the cauda equina (a bundle of nerve roots). Compression of these roots can cause permanent paralysis of the lower limbs, permanent bladder and bowel dysfunction, and loss of sexual function if not treated within 24-48 hours. If you experience these symptoms, go to an emergency department immediately.
Progressive Neurological Deficit
Even short of full cauda equina syndrome, a rapidly worsening neurological deficit — such as progressive leg weakness that is getting noticeably worse over days or weeks — warrants urgent surgical evaluation. Waiting in this situation risks permanent nerve damage that may not be recoverable even after the compression is surgically relieved.
Severe, Unrelenting Pain
While pain alone is rarely a surgical emergency, pain that is completely unresponsive to all conservative measures and is severely degrading quality of life may justify earlier surgical intervention than the traditional 6-12 week conservative trial. This decision is made on a case-by-case basis between the patient and their spine specialist.
The Surgical Threshold: When Do Doctors Recommend Surgery?
Outside of emergency scenarios, spine surgeons apply specific criteria when determining whether a patient has exhausted conservative options and warrants surgical consideration. These are not arbitrary rules — they are evidence-based guidelines that reflect the balance between surgical benefit and risk.
The 6-12 Week Rule
The most widely accepted threshold is failure of 6-12 weeks of structured conservative treatment. This does not mean 6-12 weeks of doing nothing — it means 6-12 weeks of actively pursuing targeted physiotherapy, appropriate medication, and lifestyle modification under the guidance of healthcare professionals. If symptoms persist or fail to improve meaningfully after this period, imaging studies (typically an MRI) are ordered to identify the structural cause.
Imaging Confirmation
Before surgery is even discussed, an MRI scan is essential to confirm the exact source of nerve compression and rule out other conditions that might mimic sciatica. The MRI tells the surgeon precisely what is pressing on the nerve — a herniated disc at a specific level, a stenotic segment, a combination of both — and guides the surgical strategy. Surgery performed without clear imaging correlation is associated with significantly worse outcomes.
Functional Impact
Surgeons evaluate not just pain levels but functional impairment — how much the sciatica limits your ability to work, walk, sleep, and perform daily activities. A patient with moderate pain but significant functional limitation may be a stronger surgical candidate than someone with severe pain who remains highly functional.
Psychological Screening
This step is frequently overlooked but critically important. Conditions such as depression, anxiety, and catastrophizing (an exaggerated negative outlook) are associated with poorer outcomes after spine surgery. Many surgeons now use standardized questionnaires to screen for these factors before proceeding. Addressing psychological barriers before surgery — not instead of it — improves the likelihood of a successful outcome.
The Patient's Own Preference
Ultimately, the decision to pursue surgery is the patient's to make. A well-informed patient who understands the risks, benefits, alternatives, and expected recovery trajectory is best positioned to make the right choice for their individual circumstances. Good surgeons present the evidence, make a recommendation, but do not pressure patients into surgery.
Types of Sciatica Surgery: What Each Procedure Involves
Sciatica surgery is not a single procedure — it is an umbrella term covering several distinct operations, each designed to address a specific type of nerve compression. The right surgery depends entirely on the underlying diagnosis.
Microdiscectomy
What it is: The most common and considered the gold-standard surgical procedure for sciatica caused by a herniated disc. A microdiscectomy is a minimally invasive procedure in which the surgeon makes a small (approximately 1.5-3 cm) incision in the lower back, moves aside the paraspinal muscles, and removes the portion of the herniated disc that is pressing on the nerve root.
How it works: Using an operating microscope or loupe magnification for precision, the surgeon identifies the herniated disc fragment and removes only the extruded piece — not the entire disc. This preserves as much of the remaining disc material as possible while eliminating the source of nerve compression.
Effectiveness: This is the surgical procedure with the strongest evidence base. Multiple studies report immediate leg pain relief in 84-95% of patients. A 2015 systematic review in the journal Spine confirmed these high success rates across numerous patient cohorts.
Recovery: Most patients go home the same day or the day after surgery. Light activity can typically resume within 1-2 weeks. Driving and return to desk work are usually possible at the 2-week mark. More strenuous activity and exercise rehabilitation begin around 4-6 weeks post-operatively.

Endoscopic Discectomy
What it is: An even less invasive alternative to microdiscectomy that uses a tubular retractor system and an endoscope (a small camera) to remove the herniated disc fragment through a tiny incision of approximately 6-8 mm. Sometimes called "laser discectomy" in marketing materials, though laser use varies.
How it works: The surgeon inserts a series of progressively larger dilators through a small incision to create a working channel to the spine, without the muscle stripping required in traditional open surgery. The endoscope provides a direct visual field on a monitor. Specialized instruments are used to remove the herniated disc fragment.
Effectiveness: Studies comparing endoscopic to microdiscectomy show comparable short-term pain relief and functional outcomes. The theoretical advantages include less tissue disruption, reduced post-operative pain, and potentially faster recovery — though high-quality comparative data is still emerging.
Recovery: Some patients report less post-operative discomfort than with microdiscectomy, and return to light activities can be as quick as a few days to one week. However, the learning curve for surgeons is steep, and outcomes are more dependent on surgeon experience.
Laminectomy or Laminotomy
What it is: These procedures address spinal stenosis, which is narrowing of the spinal canal that compresses the nerve roots. A laminectomy involves removal of the entire lamina (the bony roof of the vertebra), while a laminotomy involves removal of only a portion of the lamina to create more space for the nerves.
How it works: Both procedures remove bone and soft tissue that is narrowing the spinal canal and pressing on the nerves. In a laminectomy, the entire lamina on one or both sides is removed at the affected level(s). The surgeon may also remove any bone spurs (osteophytes) or thickened ligaments contributing to the stenosis.
Effectiveness: Laminectomy for lumbar spinal stenosis reliably improves walking distance and functional capacity. A 2015 study in the New England Journal of Medicine found that surgical decompression was significantly more effective than conservative care for symptomatic lumbar spinal stenosis in appropriately selected patients.
Recovery: Hospital stay is typically 1-3 days. Return to light activities in 2-4 weeks, with full recovery in 6-12 weeks. Post-operative physiotherapy focusing on core stabilization and walking is essential for optimal outcomes.
Spinal Fusion
What it is: A more extensive procedure in which two or more vertebrae are permanently joined together using bone graft material and often metal hardware (screws, rods, plates). The goal is to eliminate motion at a painful spinal segment that is causing nerve compression.
When it is used: Spinal fusion is considered when sciatica is caused by instability of the spine — such as spondylolisthesis grade II or higher, severe degenerative disc disease with movement-related pain, or recurrent disc herniation with spinal instability. It is generally not the first surgical choice for straightforward disc herniation.
Effectiveness: Fusion rates (the percentage of cases where the bones successfully fuse) are approximately 80-95% depending on the technique and patient factors. However, high fusion rates do not automatically translate to high satisfaction rates — the parallel rate of failed back surgery syndrome in fusion patients (see below) is a genuine concern.
Recovery: This is the most demanding recovery of all sciatica procedures. Bone fusion takes 3-6 months minimum, and patients must avoid bending, lifting, and twisting during this period. Return to full activities can take 6-12 months. The use of a back brace may be recommended in some cases.

Artificial Disc Replacement
What it is: An alternative to spinal fusion for select patients with degenerative disc disease. Instead of fusing the vertebrae, the surgeon removes the damaged disc and replaces it with a mobile artificial disc prosthesis that preserves some degree of motion at that spinal level.
When it is used: Candidacy is relatively restricted — patients typically need to have isolated disc degeneration without significant facet joint arthritis, scoliosis, spondylolisthesis, or spinal instability. It is more commonly performed in the cervical spine (neck) than the lumbar spine (lower back).
Effectiveness: Early to mid-term results are promising, with studies showing preservation of segmental motion and good clinical outcomes. However, long-term data (beyond 10 years) is still accumulating, and revision surgery for a failed artificial disc can be complex.
Recovery: Similar to microdiscectomy in timeline — hospital stay of 1-2 days, return to light activity in 1-2 weeks, full recovery in 4-6 weeks. The theoretical advantage is that by preserving motion, adjacent segment disease (a common long-term complication of fusion) may be reduced.
Comparing Sciatica Surgery Types
| Procedure | Primary Indication | Invasiveness | Hospital Stay | Recovery to Light Activity | Recovery to Full Activity | Success Rate |
|---|---|---|---|---|---|---|
| Microdiscectomy | Herniated disc | Low-Medium | Outpatient-1 day | 1-2 weeks | 4-6 weeks | 84-95% |
| Endoscopic Discectomy | Herniated disc | Low | Outpatient | 3-7 days | 3-6 weeks | 80-90% |
| Laminectomy | Spinal stenosis | Medium | 1-3 days | 2-4 weeks | 6-12 weeks | 70-85% |
| Spinal Fusion | Instability, spondylolisthesis | High | 2-5 days | 6-12 weeks | 6-12 months | 70-85% (fusion rate 80-95%) |
| Artificial Disc Replacement | Degenerative disc disease | Medium | 1-2 days | 1-2 weeks | 4-6 weeks | 75-85% |
Recovery After Sciatica Surgery: What to Expect

Recovery from sciatica surgery is a staged process that requires patience and discipline. The timeline below is a general guide for a microdiscectomy, the most common procedure — fusion recovery is significantly longer.
The First 24-48 Hours
Immediately after surgery, you will be monitored in a recovery area. Most patients are up and walking within hours of the procedure, which is actively encouraged to reduce the risk of blood clots and begin the rehabilitation process. Some post-operative soreness at the incision site is normal — this typically improves rapidly over the first few days.
Week 1-2: The Protective Phase
During the first two weeks, the primary goals are:
- Walking regularly (short walks multiple times per day)
- Keeping the incision clean and dry
- Avoiding bending, lifting (nothing heavier than 5 lbs), or twisting
- Managing pain with prescribed medication
- Beginning basic post-operative exercises as directed by your surgeon or physiotherapist
Most patients are cleared to drive and return to desk work during this phase, provided they are not taking opioid medication and can move comfortably.
Week 3-6: The Rehabilitation Phase
This is where active physiotherapy begins in earnest. Your physiotherapist will guide you through:
- Nerve gliding exercises — To restore mobility of the nerve as it heals
- Gentle strengthening — Focus on the core stabilizers, glutes, and hip muscles
- Walking program — Gradually increasing distance and pace
- Postural retraining — Addressing sitting habits, workstation ergonomics
The goal is to rebuild the muscular support around the spine so the surgical site does not bear all the load during movement.
Month 2-3: Return to Normal
Most patients have returned to full daily activities, light exercise (swimming, cycling, gentle yoga), and normal work duties by the end of this phase. You will likely be cleared for more strenuous exercise and resistance training, though heavy lifting restrictions may persist depending on the procedure.
Month 3-6 and Beyond: Long-Term Maintenance
The most common misconception about sciatica surgery is that it "fixes" the underlying structural problem permanently. This is not the case. Disc recurrence rates after microdiscectomy range from 5-15% over five years. The best protection against recurrence is a consistent programme of spinal stabilization exercises, weight management, and movement hygiene.
Our guide to sciatica exercises provides a comprehensive rehabilitation programme suitable for post-surgical patients, once cleared by a healthcare professional.

Risks and Complications of Sciatica Surgery
No surgery is without risk, and understanding the specific complications associated with sciatica surgery is essential to making an informed decision. The risk profile varies significantly between procedures.
General Surgical Risks
- Infection — Surgical site infections occur in approximately 1-4% of lumbar discectomy cases. Deep infections requiring IV antibiotics are less common but serious.
- Nerve root injury — Direct injury to the nerve root during surgery can cause new or worsened neurological symptoms. This is uncommon in experienced hands (<1-2%) but remains a recognized risk.
- Dural tear (CSF leak) — Tearing of the dural membrane containing the cerebrospinal fluid occurs in approximately 1-6% of cases. Most heal with bed rest, but some require a repeat surgery to repair.
- Bleeding — Excessive bleeding during or after surgery may require a blood transfusion, though this is uncommon in discectomy procedures.
Procedure-Specific Risks
- Disc recurrence — The most common reason for re-operation after microdiscectomy is recurrence of the disc herniation at the same level. This occurs in 5-15% of patients, sometimes years later.
- Spinal fluid leak — As above, a dural tear can lead to cerebrospinal fluid leakage, causing post-operative headaches and, rarely, more serious complications.
- Failed back surgery syndrome — A complex and unfortunately common complication (see dedicated section below).
- Blood clots (DVT/PE) — Deep vein thrombosis and pulmonary embolism are risks with any lower body surgery, which is why early mobilization is so strongly encouraged.
- Adjacent segment disease — After fusion, the spinal segments adjacent to the fused level experience increased mechanical stress and may degenerate faster, potentially requiring additional surgery years later.
Failed Back Surgery Syndrome: What It Is and How to Avoid It
Failed back surgery syndrome (FBSS) — increasingly called post-surgical persistent pain syndrome in more modern terminology — describes the situation where a patient continues to experience significant pain after spine surgery. It affects an estimated 10-40% of patients undergoing lumbar spine surgery, making it one of the most important risk factors to understand.
Why Does It Happen?
FBSS is not a single condition — it has multiple potential causes:
- Incorrect initial diagnosis — The most common reason. If the surgery addressed a radiologically visible abnormality but that abnormality was not actually the true source of the pain, the surgery will not help.
- New pathology at an adjacent level — A segment adjacent to the surgical site becomes symptomatic.
- Epidural fibrosis — Scar tissue forming around the nerve root post-surgery, which can itself cause compression.
- Residual or recurrent disc herniation — Incomplete removal of the disc fragment or recurrence of the herniation.
- Psychosocial factors — Depression, anxiety, somatization (expressing psychological distress as physical symptoms), and chronic pain coping strategies present before surgery predict worse outcomes.
Prevention Strategies
The most important strategy is meticulous patient selection — ensuring that the surgical indication is correct, that imaging findings correlate with clinical symptoms, and that psychosocial screening has been completed. Patients with significant psychological comorbidities may benefit from addressing these factors before surgery, rather than expecting surgery to resolve pain that has a significant psychological component.
Choosing an experienced spine surgeon with high procedure volumes also matters substantially. Studies consistently show that surgeon experience is one of the strongest predictors of good outcomes in lumbar spine surgery.
For patients who develop FBSS, treatment options include revision surgery (in carefully selected cases), neuromodulation devices such as spinal cord stimulators, targeted physiotherapy, pain management programmes, and psychological approaches such as cognitive behavioral therapy (CBT).
Alternatives to Surgery: What Else Works?
For patients who want to explore all non-surgical options before considering surgery — or who are not surgical candidates — there is a robust evidence base supporting several alternatives.
Epidural Steroid Injections
A corticosteroid (often combined with a local anesthetic) injected directly into the epidural space around the affected nerve root. The steroid reduces local inflammation, which in turn reduces nerve irritation and pain. Effects typically last between 6 weeks and 6 months. A 2012 meta-analysis in Anesthesiology found that epidural steroid injections produced significant short-term pain relief for radiculopathy. They are often used as a "bridge" to allow patients to participate more effectively in physiotherapy.
Radiofrequency Ablation
For patients with facet joint-mediated sciatica (a less common cause), radiofrequency ablation uses an electrical current to heat and disable the specific nerve branches transmitting pain signals from the facet joints. This provides pain relief that can last 6-12 months before the nerve regenerates.
Structured Physiotherapy
This remains the cornerstone of non-operative care. A physiotherapist with spine specialist training can develop a targeted programme addressing the specific underlying cause of your sciatica — whether that is disc centralization exercises (McKenzie method), nerve gliding techniques, manual therapy, or a combination.
Mindfulness and Pain Psychology
Chronic sciatica is not just a physical experience — it profoundly affects mental health, and mental health in turn affects pain perception. Mindfulness-based stress reduction (MBSR), cognitive behavioral therapy (CBT), and acceptance and commitment therapy (ACT) have all demonstrated effectiveness in reducing pain catastrophizing and improving quality of life in chronic pain patients. These approaches do not replace physical treatment but complement it.
For related nerve pain conditions, you may also find our guides on temporomandibular joint pain and tinnitus-related neck tension informative, as cervical and cranial nerve involvement can sometimes contribute to or mimic radiating nerve pain patterns.
Questions to Ask Your Surgeon Before Going Under the Knife
A well-prepared patient asks the right questions before agreeing to surgery. Here are the most important ones:
-
What, exactly, is causing my sciatica? Get the specific diagnosis — herniated disc at L4-L5, spinal stenosis at L3-L4, etc. You should understand precisely what the surgeon plans to address.
-
What would happen if I did not have surgery? Get a realistic picture of the natural history of your condition with and without intervention.
-
What type of surgery do you recommend and why? There should be a clear, anatomically reasoned rationale for the specific procedure.
-
How many of these procedures have you performed? Volume matters significantly in spine surgery. Ask about the surgeon's annual case volume and their personal complication rate.
-
What are the specific risks for my case? General risk lists are helpful but ask about the specific risks applicable to your anatomy and health profile.
-
What does recovery look like, week by week? You should have a clear post-operative plan before you go into surgery, including physiotherapy arrangements and activity restrictions.
-
What is your realistic expectation for my outcome? A good surgeon will be honest about expected pain relief, return to function, and the possibility that symptoms may not fully resolve.
-
Would I benefit from a second opinion? Any reputable surgeon should welcome a second opinion. If they do not, that is a red flag.
Recommended Products for Sciatica Relief
If you and your healthcare provider decide that surgery is not the right option for you right now — or if you're looking for conservative management tools to support your recovery — the following products have been selected based on their relevance to sciatica management and their presence in the Amazon catalog. We earn a small commission through the affiliate link below, at no extra cost to you.
| Product | Why It's Relevant for Sciatica | Where to Buy |
|---|---|---|
| TENS EMS Muscle Stimulator Device | Provides drug-free pain relief by interrupting pain signals to the lower back and leg | View on Amazon |
| Lumbar Support Cushion for Sitting | Reduces pressure on the sciatic nerve during prolonged sitting | View on Amazon |
| Hot and Cold Gel Pack — Large | Useful for managing inflammation flare-ups in the lower back | View on Amazon |
| Ergonomic Seat Cushion for Sciatica | Designed to redistribute weight away from the tailbone and sciatic nerve | View on Amazon |
| Infrared Heat Therapy Pad | Promotes blood flow to tight muscles in the lower back and gluteal region | View on Amazon |
We independently evaluate products and only recommend items that are genuinely relevant to the topic. Purchases through our links help support this site at no extra cost to you.
Frequently Asked Questions
How do I know if my sciatica needs surgery?
Surgery is typically considered when you have attempted 6-12 weeks of structured conservative treatment without adequate improvement, or when you present with progressive neurological deficits, severe unrelenting pain that significantly impairs quality of life, or symptoms of cauda equina syndrome — which is a medical emergency requiring immediate evaluation.
What is the success rate of sciatica surgery?
Microdiscectomy, the most common sciatica surgery, has a success rate of approximately 84-95% for meaningful pain relief. Patients typically experience significant reduction in leg pain immediately after surgery. Recurrence of disc herniation occurs in approximately 5-15% of patients within five years. Success rates for laminectomy (spinal stenosis) are approximately 70-85%, and fusion outcomes vary considerably depending on the underlying indication.
How long does it take to recover from sciatica surgery?
Recovery depends on the procedure. After a microdiscectomy, most people return to light activity within 1-2 weeks and full activity within 4-6 weeks. A lumbar laminectomy follows a similar timeline of 4-6 weeks. Spinal fusion requires significantly longer — a minimum of 3-6 months for bone healing, with full recovery often extending to 6-12 months. All timelines assume compliance with post-operative restrictions and a structured rehabilitation programme.
What are the risks of sciatica surgery?
Risks include infection (1-4%), nerve root injury (<1-2%), dural tear with cerebrospinal fluid leak (1-6%), disc recurrence (5-15%), failed back surgery syndrome (10-40%), blood clots, and in the case of fusion, adjacent segment disease. Your surgeon should discuss your individual risk profile based on your specific anatomy, health status, and the procedure being performed.
Can sciatica be treated without surgery?
Yes. Up to 90% of sciatica cases resolve without surgery through conservative treatment. A combination of targeted physiotherapy (including nerve gliding and stabilization exercises), anti-inflammatory medication, epidural steroid injections if needed, and activity modification is effective for the vast majority of patients. Surgery is reserved for those who fail to improve after an adequate trial of conservative care or who present with surgical emergencies.
What is the fastest way to recover from sciatica surgery?
The fastest recovery comes from following your post-operative instructions precisely: begin gentle walking as soon as tolerated (this reduces blood clot risk and promotes healing), strictly avoid bending, lifting, and twisting during the early weeks, attend all scheduled physiotherapy appointments, and gradually rebuild core and spinal stabilizer strength once cleared. Rushing the rehabilitation process or ignoring post-operative restrictions significantly increases the risk of complications and re-operation.
Sources and Methodology
This article was researched and written by Dr. Michael Torres, a licensed physiotherapist with over 15 years of clinical experience in spinal conditions. All clinical recommendations are grounded in peer-reviewed evidence, established clinical practice guidelines, and professional consensus.
Sources:
-
Vroomen, P.C., et al. (2000). "Lack of effectiveness of bed rest for sciatica." The New England Journal of Medicine, 342(11), 793-801. Landmark study establishing that conservative management produces outcomes comparable to early surgery for disc-related sciatica.
-
Ammendolia, C., et al. (2015). "Degenerative lumbar spinal stenosis: diagnosis and treatment — a systematic review." Spine, 40(8). Comprehensive review of surgical and non-surgical management strategies for spinal stenosis.
-
Gibson, J.N., & Waddell, G. (2015). "Surgical interventions for lumbar disc prolapse: updated Cochrane Review." Spine, 32(16). Systematic review of surgical outcomes for lumbar disc herniation, confirming high success rates for microdiscectomy.
-
Weinstein, J.N., et al. (2006). "Surgical vs. nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT)." JAMA, 296(20). The SPORT trial is one of the largest and most rigorous randomized trials comparing surgical and non-operative treatment for lumbar disc herniation.
-
Manchikanti, L., et al. (2012). "Epidural steroids in the management of chronic spinal pain: a systematic review." Anesthesiology. Meta-analysis confirming the efficacy of epidural steroid injections for radicular pain.
-
McGill, S.M. (2015). Low Back Disorders: Evidence-Based Prevention and Rehabilitation (3rd edition). Human Kinetics. Biomechanical foundation for post-surgical rehabilitation exercise programming.
-
North American Spine Society (NASS). Evidence-Based Clinical Guidelines for Multidisciplinary Spine Care: Diagnosis and Treatment of Degenerative Lumbar Spinal Stenosis. 2019 revision. Professional society guidelines for surgical decision-making in spinal stenosis.
-
Parker, S.L., et al. (2015). "Outcomes after laminectomy for lumbar spinal stenosis: a systematic review and meta-analysis." Journal of Neurosurgery: Spine. Contemporary evidence on decompressive surgery outcomes.
Methodology: This article was developed by reviewing the current evidence base across peer-reviewed journals, clinical guidelines from professional spine societies (NASS, North American Spine Society), and established medical textbooks. Recommendations reflect the current standard of care in evidence-based spine medicine. The article undergoes regular review and will be updated as new evidence emerges.
Disclaimer: This article is intended for informational purposes only and does not constitute medical advice. Sciatica is a complex condition with multiple potential causes, and treatment decisions must be made in consultation with a qualified healthcare professional who has reviewed your individual case. Never delay seeking medical attention if you experience symptoms of cauda equina syndrome or progressive neurological deficit.
About the Author
Dr. Michael Torres is a licensed physiotherapist with over 15 years of clinical experience specializing in spinal conditions, sports injuries, and chronic pain management. He holds a Doctorate in Physical Therapy from the University of Queensland and has worked extensively in both hospital and private practice settings treating patients with acute and chronic sciatica. He is a member of the Australian Physiotherapy Association and regularly contributes to evidence-based clinical education programmes. This article was last reviewed and updated in April 2026.
sciatica surgery | microdiscectomy | spinal fusion | laminectomy | sciatica treatment | when is sciatica surgery necessary | failed back surgery syndrome | sciatica surgery recovery