Sciatica Relief
Sciatica From Sitting Too Long: Causes, Relief & Prevention (2026)
Prolonged sitting compresses the sciatic nerve and triggers painful flare-ups. Learn exactly why it happens and 7 proven relief strategies for desk workers in 2026.
Prolonged sitting raises lumbar disc pressure by up to 90%, tightens the piriformis muscle over the sciatic nerve, and shortens hip flexors that tilt the pelvis forward. The result is the burning, shooting leg pain of a sciatica flare-up. Most desk workers can break this cycle with correct seated posture, regular movement breaks, and targeted daily stretches.
Last updated: April 2026 | By Dr. Sarah Mitchell, Physical Therapist
Affiliate disclosure: This article contains affiliate links. We may earn a commission at no extra cost to you.
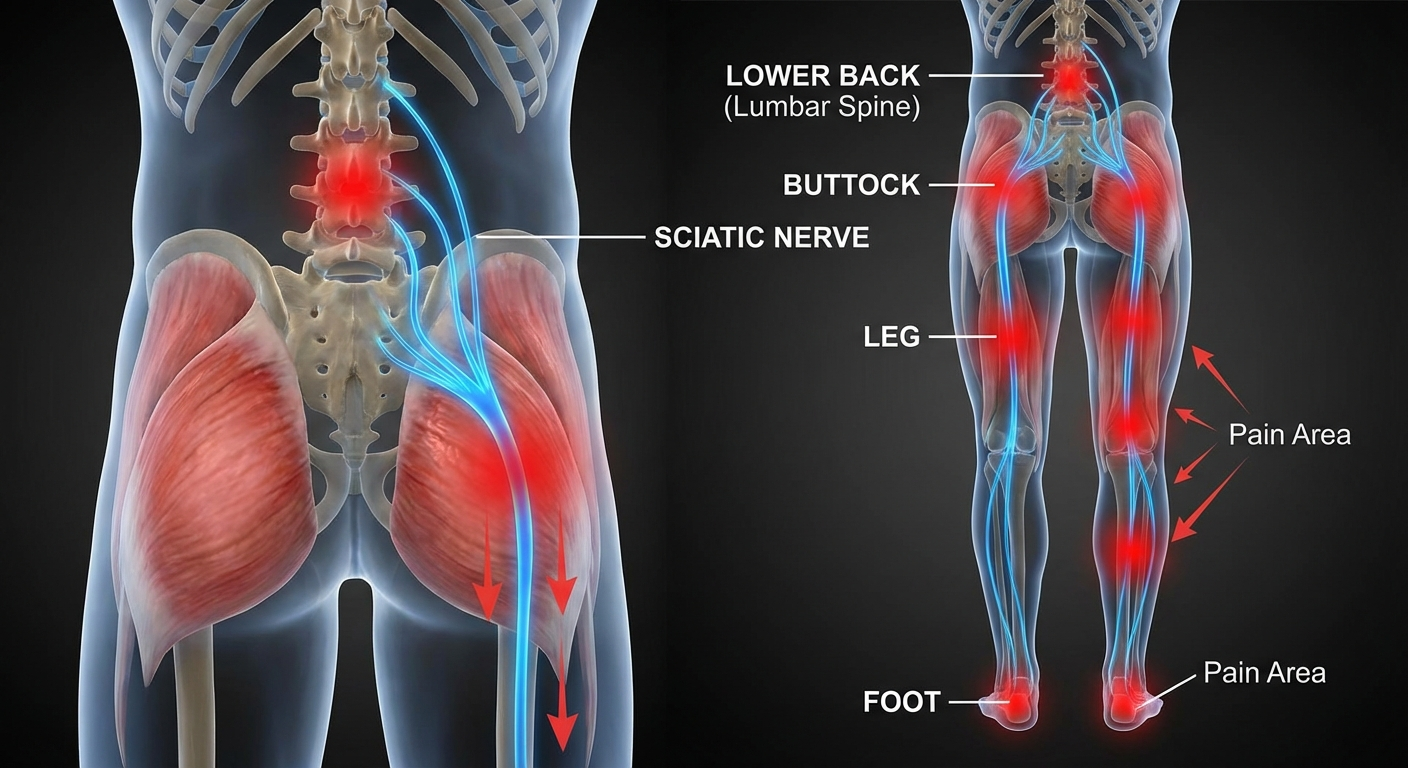
If you spend most of your working day sitting at a desk, you already know the pattern: a dull ache creeps into your lower back after lunch, a familiar tingle begins down one buttock and leg, and by 4 PM you are shifting constantly in your chair trying to find relief. This is sitting-triggered sciatica, and it affects millions of desk workers, drivers, and students worldwide.
The good news is that sciatica from sitting is one of the most manageable forms of this condition. Unlike sciatica caused by severe disc extrusion or spinal stenosis, sitting-triggered flare-ups respond quickly to the right combination of posture changes, movement habits, and targeted exercises. This guide explains exactly what happens in your spine when you sit too long, the warning signs to watch for, and seven specific strategies to get relief today.
Table of Contents
- Why Sitting Triggers Sciatica
- Warning Signs Your Sitting Is Making It Worse
- 7 Immediate Relief Strategies
- Ergonomic Setup for Sciatica Sufferers
- Daily Habits to Prevent Flare-Ups
- When to See a Doctor
- Frequently Asked Questions
- Sources & Methodology
Why Sitting Triggers Sciatica
Understanding the mechanics of sitting-triggered sciatica makes it easier to take the right action. There are four distinct physiological changes that occur when you sit for extended periods, and each one can independently compress or irritate the sciatic nerve.
The Lumbar Disc Pressure Problem
The foundational research here was published by Alf Nachemson in 1981 in Spine, measuring actual intradiscal pressure in living subjects across different postures. His findings remain the gold standard in spinal biomechanics: when you sit in an unsupported, slightly forward-leaning position, lumbar disc pressure increases to approximately 150% of the standing load. Even well-supported seated posture produces about 40% more disc pressure than standing.
Why does this matter for sciatica? The L4-L5 and L5-S1 intervertebral discs are the most common sites for herniation — and they sit directly adjacent to the sciatic nerve roots. When disc pressure rises from sustained sitting, the disc material is pushed posteriorly, toward the nerve root. Over hours of sitting, this mechanical load slowly increases nerve root compression and inflammation.
The process is worsened by what biomechanists call viscoelastic creep: spinal ligaments and discs gradually deform under sustained load. After 20 minutes of poor sitting posture, your lumbar ligaments have elongated enough that they can no longer stabilise the spine effectively. The discs are then bearing disproportionate load, narrowing the safety margin before nerve compression occurs.
The Piriformis Squeeze
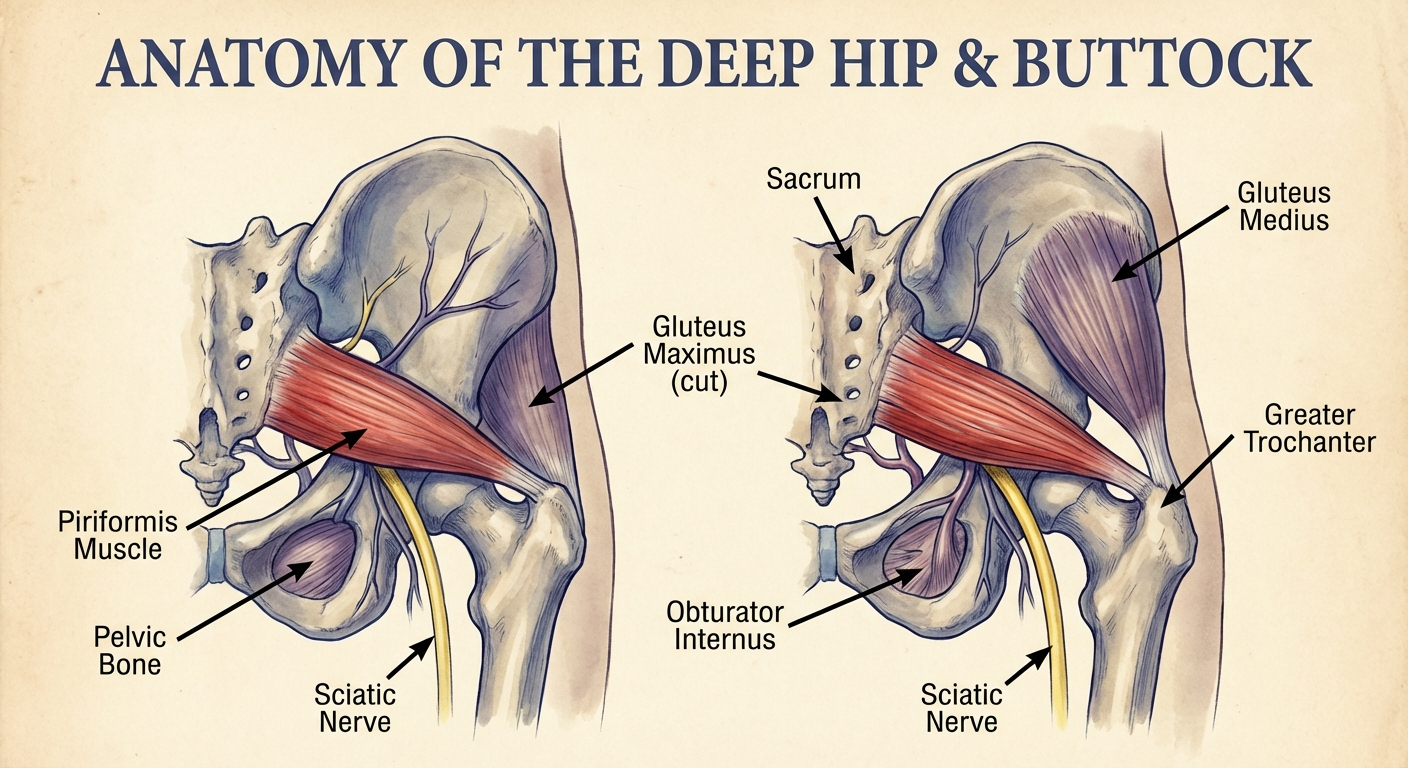
The piriformis is a small, pear-shaped muscle that sits deep in the buttock, connecting the sacrum to the top of the femur. It is responsible for externally rotating the hip. What makes it clinically important for sciatica is its relationship to the sciatic nerve: in approximately 83% of people, the sciatic nerve passes directly beneath the piriformis. In the remaining 17%, the nerve passes through the muscle itself.
When you sit for extended periods, the piriformis is held in a shortened position and often under sustained compression from the chair surface. Over time, it can tighten, spasm, or develop trigger points that squeeze the adjacent sciatic nerve. This is sometimes called piriformis syndrome, and it can produce symptoms that are identical to disc-related sciatica.
Hip Flexor Tightening and Anterior Pelvic Tilt
The hip flexor muscles — primarily the iliopsoas and rectus femoris — attach from the front of the lumbar vertebrae to the top of the femur. When you sit, these muscles are held in a shortened position for hours at a time. Sustained shortening causes adaptive tightening, which pulls the top of the pelvis forward in a pattern called anterior pelvic tilt.
This forward tilt does two damaging things simultaneously: it increases the lumbar lordotic curve (arch of the lower back) beyond its neutral position, compressing the posterior disc margins; and it creates an imbalanced loading pattern across the lumbar vertebrae that concentrates stress at the L4-L5 and L5-S1 levels.
The result is a posture where every subsequent sitting session starts with already-shortened hip flexors — and the mechanical load on the sciatic nerve roots is already elevated before you even open your laptop.
Reduced Blood Flow and Nerve Sensitisation
The fourth mechanism is often overlooked: sustained sitting compresses the soft tissues of the buttock, reducing blood flow to the sciatic nerve and surrounding structures. Nerves are metabolically demanding — they require a continuous supply of oxygen and nutrients. When circulation is restricted, inflammatory mediators accumulate around the nerve, lowering its firing threshold and amplifying pain signals.
This is why sciatica pain from sitting often has a burning or hypersensitive quality in addition to the mechanical shooting pain. The nerve has been made chemically sensitive, not just mechanically compressed.
Warning Signs Your Sitting Is Making It Worse
Recognising the early warning signs of sitting-triggered sciatica allows you to intervene before a minor irritation becomes a debilitating episode.
Progressive Pain Patterns to Watch
The following patterns indicate that your sitting habits are actively worsening your sciatic nerve situation:
- Pain that builds predictably throughout the day: If you feel fine in the morning and progressively worse by afternoon, cumulative disc loading from sitting is almost certainly a factor.
- Stiffness or ache when first standing up: This indicates the lumbar ligaments and discs have adapted to the flexed seated position — it takes a moment for the spine to return to a neutral load distribution.
- Pain that radiates further down the leg as the day progresses: A symptom that starts in the buttock but extends into the thigh, calf, or foot over the course of a working day suggests increasing nerve compression.
- Relief when walking but return of pain when sitting again: This classic pattern — improvement with movement, worsening with sitting — is strongly associated with sitting-triggered disc-related sciatica.
- Tingling or numbness in the foot or toes after long sitting periods: Persistent pins and needles in the extremity of the affected leg indicates significant nerve root compression.
5 Sitting Habits That Silently Worsen Sciatica
Beyond just sitting too long, specific habits accelerate nerve compression:
1. Wallet in the back pocket. A wallet under one buttock creates an uneven pelvic tilt that compresses the sciatic nerve on that side. This is sometimes called "wallet sciatica" or "back pocket sciatica." Remove your wallet before sitting — every time.
2. Leg crossing. Crossing one leg over the other shifts body weight asymmetrically onto the sacrum, rotates the pelvis, and tightens the piriformis on the crossed side. It also creates vascular compression in the thigh that affects nerve nutrition.
3. Sitting on soft, unsupported surfaces. Sofas and most car seats without lumbar support allow the pelvis to roll backward (posterior tilt), eliminating the natural inward curve of the lumbar spine. This flattening dramatically increases disc pressure at the L4-L5 and L5-S1 levels.
4. Forward lean toward a screen. When you lean your upper body forward toward your monitor, you shift your centre of mass in front of your spinal column. The lower back muscles must fire continuously to hold you up, increasing compressive load at the lumbar discs substantially.
5. Sitting without breaks for more than 45 minutes. Even perfect posture in a perfect chair produces cumulative disc loading when maintained without interruption. The 30 to 45 minute sitting interval is not arbitrary — it reflects the time it takes for viscoelastic creep to significantly compromise spinal ligament stability.
7 Immediate Relief Strategies
When sciatica flares up from prolonged sitting, these seven strategies provide the most reliable immediate relief. Apply them in the order listed for best results.
1. Get Up and Walk Gently
The single most effective immediate response to a sitting-triggered sciatica flare is to stand up and walk slowly. Walking is mechanically the opposite of sitting: it alternates lumbar flexion and extension, reduces disc pressure compared to sitting, and promotes blood flow to the compressed nerve root.
Even a 5-minute walk at a slow, gentle pace encourages fluid exchange in the discs, loosens tight piriformis and gluteal muscles, and interrupts the cycle of nerve sensitisation that builds up during prolonged sitting. Do not walk through sharp, shooting pain — if symptoms are severe, walk slowly and only until the acute pain begins to ease.
2. McKenzie Press-Up
Developed by New Zealand physiotherapist Robin McKenzie, this exercise is one of the most evidence-supported interventions for disc-related sciatica. The extension movement helps push disc material anteriorly, away from the nerve root — a process McKenzie called "centralisation."
How to perform:
- Lie face down on a firm surface with your hands under your shoulders, as if preparing for a press-up.
- Keeping your hips and pelvis pressed firmly into the floor, slowly push your upper body up by extending your arms.
- Allow your lower back to arch gently. Your hips must stay on the ground.
- Hold the top position for 5 to 10 seconds.
- Slowly lower back down. Repeat 10 times.
A key sign the exercise is working: pain that was in your leg should begin moving toward your lower back (centralising). If leg pain increases significantly, stop and consult a physiotherapist.
3. Standing Back Extension
This is the vertical, portable version of the McKenzie press-up. It is ideal during the workday because you can do it anywhere — at your desk, in the kitchen, or during a phone call.
- Stand with feet shoulder-width apart.
- Place both hands on your lower back, fingers pointing downward.
- Gently lean backward, arching through the lumbar spine and using your hands for support.
- Hold for 3 to 5 seconds. Repeat 10 times.
Perform this every time you stand up from your desk. It counteracts the cumulative flexion loading of sitting before it has a chance to compress the nerve root.
4. Piriformis Stretch
This stretch directly targets the piriformis muscle that can compress the sciatic nerve in the buttock.
- Lie on your back with knees bent.
- Cross the ankle of the affected leg over the opposite knee to form a figure-4 shape.
- Gently pull the uncrossed leg toward your chest until you feel a deep stretch in the buttock of the crossed leg.
- Hold for 30 to 40 seconds. Repeat 3 times per side.
You can also perform this seated at your desk: sit upright, cross the affected ankle over the opposite knee, keep your back straight, and lean gently forward from the hips until you feel the deep buttock stretch.
5. Standing Hip Flexor Stretch
This stretch addresses the hip flexor tightening from prolonged sitting that tilts the pelvis and increases lumbar disc load.
- Step one foot forward into a lunge position.
- Lower the back knee gently to the floor (use a cushion if needed).
- Push your hips gently forward and slightly downward until you feel a stretch in the front of the rear hip.
- Keep your torso upright.
- Hold 30 seconds per side. Repeat twice each side.
Doing this stretch after every hour of sitting can meaningfully reduce the cumulative hip flexor shortening that worsens sciatica over the course of a working day.
6. Nerve Flossing (Sciatic Nerve Glide)
When the sciatic nerve becomes irritated, it can develop adhesions to surrounding tissues that restrict its normal movement. Nerve flossing gently mobilises the nerve through its full range.
- Sit upright on the edge of a chair, feet flat on the floor.
- Straighten the affected leg while simultaneously tilting your head back and looking toward the ceiling.
- Then bend the knee back down while tucking your chin toward your chest.
- Alternate between these two positions in a slow, rhythmic motion — about one cycle every 3 to 4 seconds.
- Perform 10 to 15 repetitions.
This should not reproduce significant pain. If it does, reduce the range of motion or skip this exercise and consult a physiotherapist.
7. Heat Application to the Lower Back and Buttock
Apply a heat pack to the lower back and gluteal region for 10 to 15 minutes after a sitting flare-up. Heat increases blood flow to the compressed tissues, relaxes muscle spasm around the sciatic nerve, and reduces the stiffness that accumulates during prolonged sitting.
Use a warm (not hot) pack that you can hold comfortably against bare skin. The Mighty Bliss Electric Heating Pad is a popular choice among our readers for its large surface area and adjustable temperature settings. Apply heat after movement — not instead of it. Staying still with a heat pack on is less effective than using heat after a brief walk and some stretching.
Ergonomic Setup for Sciatica Sufferers
Prevention begins with your environment. The right chair setup reduces the cumulative disc load of a working day by a measurable amount. Here is how to optimise every component.
Chair Type Comparison for Sciatica Sufferers
Not all chairs provide the same protection for the sciatic nerve. This comparison covers the main options you are likely to encounter:
| Chair Type | Lumbar Support | Disc Pressure | Piriformis Pressure | Best For |
|---|---|---|---|---|
| Ergonomic office chair (adjustable lumbar) | Excellent | Low–Moderate | Low | Full-day desk work |
| Saddle chair | Natural lordosis | Low | Very Low | 2–4 hour stints, shared with regular chair |
| Kneeling chair | Moderate | Low | Low | Users with disc herniation |
| Exercise ball | None (active stability) | Moderate | Moderate | Short stints only (max 30 min) |
| Standard office chair (no lumbar) | Poor | High | Moderate–High | Not recommended for sciatica |
| Sofa / soft seating | Very Poor | Very High | High | Avoid for work |
| Standing desk | N/A | Very Low | Very Low | Alternating with sitting every 30–45 min |
Key takeaway: An ergonomic office chair with adjustable lumbar support is the best all-day option for most desk workers with sciatica. A standing desk used in alternation with sitting is the gold standard for reducing cumulative disc load across the working day.
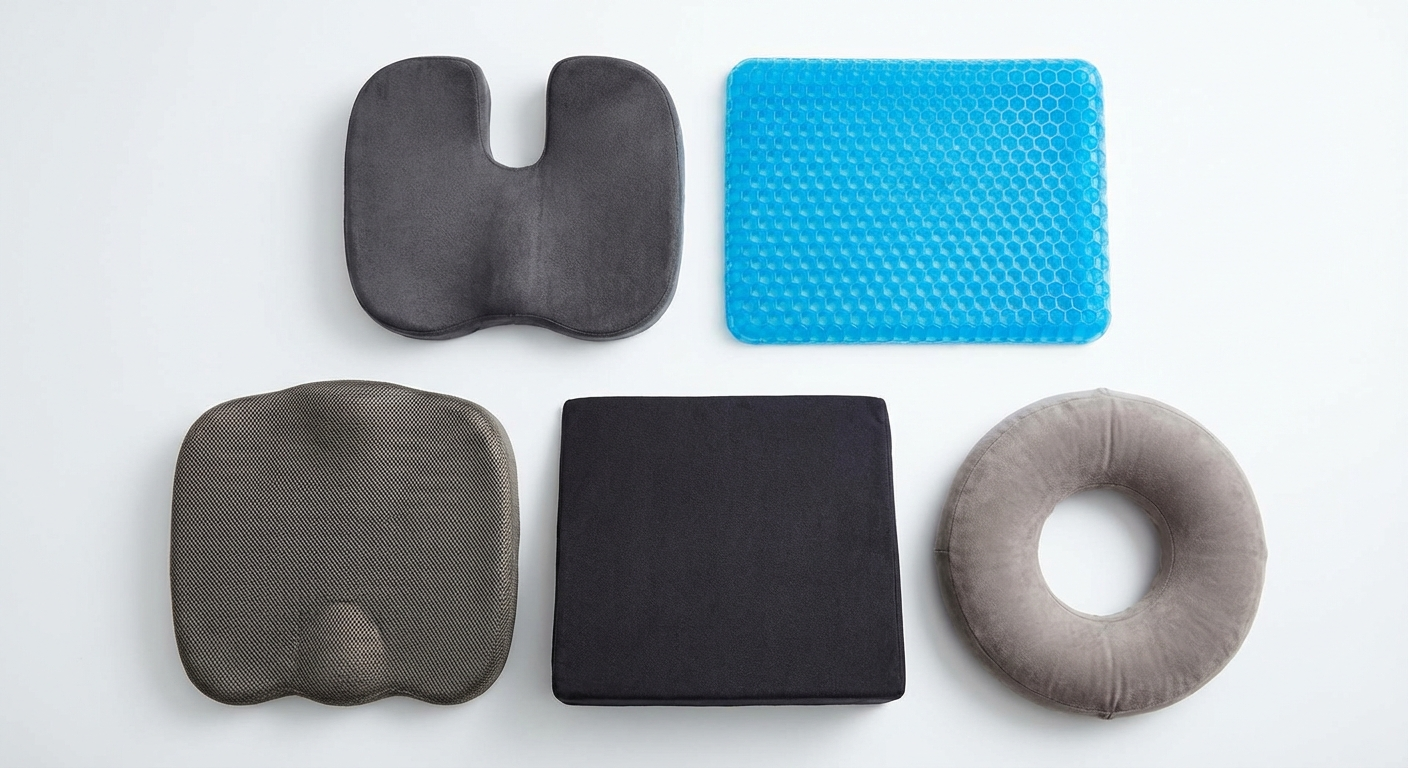
Seat Cushion Recommendations
If your chair lacks adequate support, a quality seat cushion can make a significant difference by redistributing pressure away from the sciatic nerve and promoting the lumbar curve. For a detailed comparison of the top-rated options, see our guide to the best seat cushions for sciatica in 2026.
Memory Foam Coccyx Cushion
Best for: Full-day desk sitting with disc-related sciatica
Key feature: Coccyx cutout relieves tailbone and piriformis pressure
Check on Amazon →Adjustable Lumbar Support Cushion
Best for: Chairs lacking built-in lumbar adjustment
Key feature: Maintains natural lumbar lordosis, reduces disc pressure
Check on Amazon →
Car Seat Cushion for Sciatica
Best for: Drivers and long commuters with sciatica
Key feature: Low-profile design fits car seats, non-slip base
Check on Amazon →Wedge Seat Cushion (Tilted)
Best for: Disc herniation sciatica — promotes anterior pelvic tilt
Key feature: 8–12 degree wedge maintains lumbar curve naturally
Check on Amazon →The Complete Ergonomic Checklist
Beyond the chair and cushion, these adjustments collectively reduce sciatic nerve compression during seated work:
Chair height: Feet should rest flat on the floor with knees at 90 degrees. Hips should be at or slightly above knee height. If your chair is too high, use a footrest. If too low, raise the seat.
Lumbar support position: The lumbar support (built-in or cushion add-on) should sit in the inward curve of your lower back — not at the mid-back. Many people position lumbar support too high, which pushes the thoracic spine forward without helping the lumbar region.
Screen height: The top of your monitor should be at eye level. Screens positioned too low cause you to look down, which creates a forward head posture that cascades into lumbar flexion.
Keyboard and mouse distance: Both should be within easy reach without leaning forward. Reaching for the mouse repeatedly causes subtle forward torso lean that accumulates into significant lumbar disc load over a working day.
Armrests: Set armrests so your shoulders are relaxed and arms are roughly parallel to the floor. Armrests that are too high push your shoulders up; too low causes you to lean to one side.
Sit-stand desk: For those who spend more than 5 hours per day seated, a height-adjustable sit-stand desk is one of the most evidence-supported interventions for reducing sitting-related sciatica. Aim to alternate between sitting and standing every 30 to 45 minutes.
Daily Habits to Prevent Flare-Ups
Managing sitting-triggered sciatica is not a one-time fix — it is an ongoing practice. These daily habits address the underlying vulnerabilities that sitting exploits.
The 30-Minute Movement Rule
The single most impactful habit change for most desk workers is simple: set a timer and stand up to move for 2 to 3 minutes every 30 minutes. This movement break does not need to be formal exercise. A short walk to the kitchen, a set of standing back extensions at your desk, or a brief piriformis stretch is sufficient.
What matters is interrupting the cumulative disc loading and piriformis tightening before it reaches the threshold that triggers nerve compression. Research published in the British Journal of Sports Medicine found that people who broke up sitting time with regular brief movement bouts had significantly lower rates of chronic low back pain than those who sat continuously, even when the total amount of sitting was identical.
Use your phone timer, a desktop app, or a wearable fitness tracker to enforce this habit. Most people find the discipline easier than they expect once the benefits — less pain by end of day — become apparent within the first week.
Core Strengthening for Long-Term Protection
A stable, strong core reduces the burden on the lumbar discs and sciatic nerve roots. Weak core muscles force the spinal structures themselves to bear loads that should be distributed across the deep abdominal and lumbar stabilisers.
The most evidence-supported core exercises for sciatica prevention are not crunches or sit-ups (which increase disc pressure) but the stabilisation exercises developed by spine researcher Stuart McGill:
Bird-dog: Start on all fours. Simultaneously extend one arm forward and the opposite leg backward. Hold 5 to 10 seconds. Repeat 8 times per side. This trains the deep spinal stabilisers without loading the discs.
Modified plank (forearm plank): Support yourself on forearms and toes, body straight. Hold 20 to 30 seconds. Progress to 60 seconds over several weeks.
Glute bridge: Lie on your back, knees bent, feet flat. Press through your heels to lift your hips until your body forms a straight line from shoulders to knees. Hold 5 seconds, lower slowly. Repeat 10 to 15 times. This activates the gluteus maximus, which is frequently inhibited by prolonged sitting and contributes to piriformis overload.
For a complete exercise programme with progressions, see our full guide on sciatica exercises.
Daily Walking
Walking is the most underrated preventive measure for sitting-triggered sciatica. A minimum of 20 to 30 minutes of brisk walking each day promotes disc hydration through the pumping action of alternating spinal movement, increases blood flow to the nerve roots, and maintains the hip flexor flexibility that sitting continuously erodes.
If you currently do no daily walking, start with 10 minutes and increase by 5 minutes each week. Most people notice a meaningful reduction in end-of-day sciatic symptoms within two to three weeks of establishing a daily walking habit.
Sleep Position Matters Too
The hours you spend sleeping are the longest continuous posture load your spine endures. If your sleep position forces your spine into a pain-provoking posture for 6 to 8 hours, it can undo the benefits of everything you do during the day.

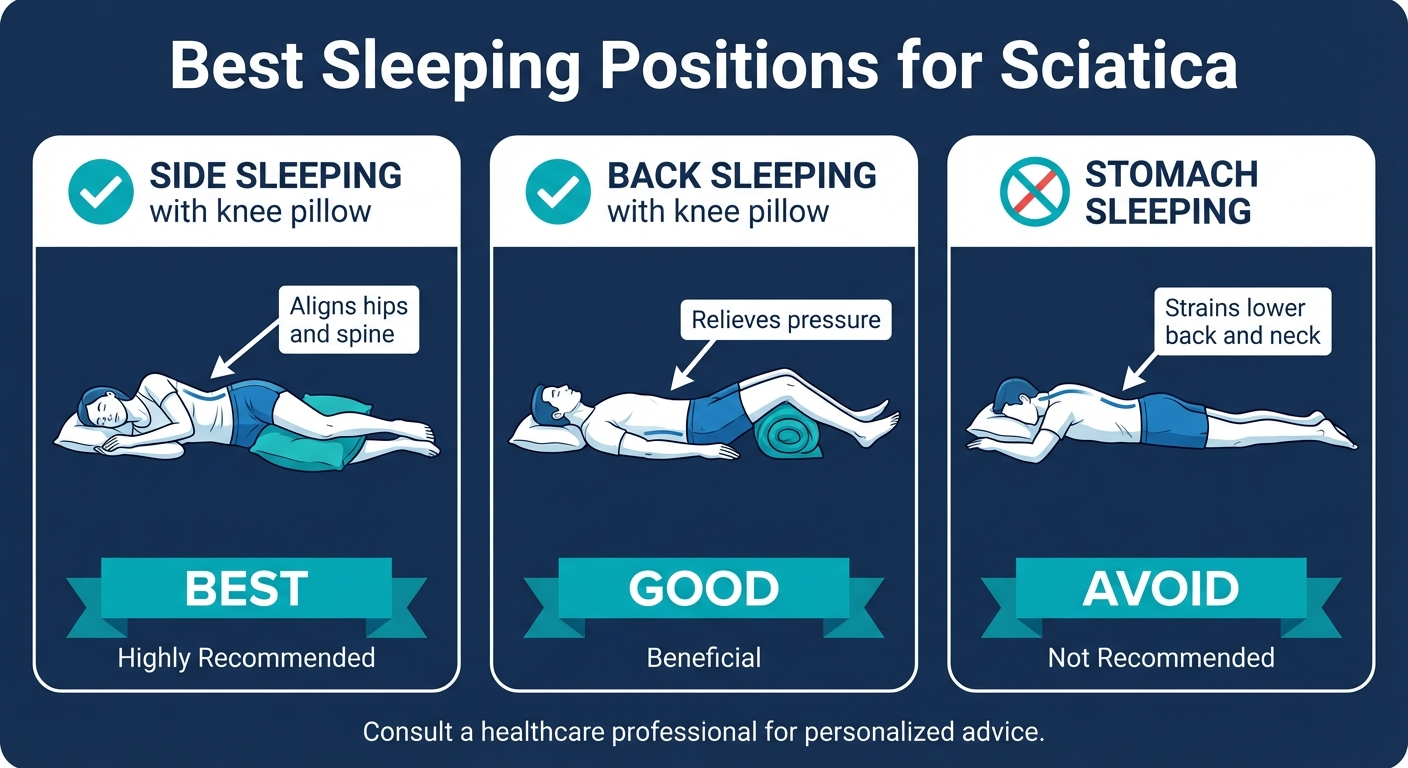
The best sleep position for sciatica is on your side with a firm pillow between your knees. This keeps your hips, pelvis, and lumbar spine in neutral alignment throughout the night, reducing nerve root compression. Back sleeping with a pillow under both knees is also beneficial.
Avoid stomach sleeping entirely — it forces the lumbar spine into hyperextension and dramatically increases posterior disc pressure. For a detailed guide on sleep positions, pillow placement, and mattress considerations, see our article on the best sleeping positions for sciatica.
Addressing Contributing Lifestyle Factors
Several lifestyle factors silently increase the baseline vulnerability of your sciatic nerve:
Body weight: Each kilogram of excess body weight adds approximately four kilograms of force to the lumbar spine during daily activities. A modest weight reduction of 5 to 10% has been shown to meaningfully reduce sciatica symptom frequency and severity.
Smoking: Nicotine constricts blood vessels and reduces nutrient delivery to the intervertebral discs, accelerating disc degeneration. Smokers have a significantly higher risk of chronic lumbar radiculopathy than non-smokers.
Stress: Psychological stress elevates cortisol and systemic inflammation, sensitises nerve tissue to pain signals, and increases paraspinal and piriformis muscle tension. Even brief daily mindfulness or breathing practices can reduce the baseline nerve sensitivity that makes sitting more likely to trigger a flare.
For a detailed breakdown of all the factors that can trigger a sciatica episode, see our guide on sciatica flare-up triggers.
When to See a Doctor
Most sciatica from prolonged sitting improves significantly within two to six weeks of consistently applying posture corrections, movement breaks, and the exercises described above. However, certain symptoms require prompt medical attention.

Seek Emergency Medical Care Immediately For:
- Loss of bladder or bowel control — this may indicate cauda equina syndrome, a surgical emergency. Do not wait. Go to an emergency department immediately.
- Numbness in the saddle area (inner thighs, groin, buttocks) — another sign of cauda equina syndrome.
- Progressive weakness in both legs — inability to lift your foot off the floor (foot drop), extreme difficulty standing or walking.
- Severe pain following a fall or accident — spinal fracture or major disc rupture needs imaging before any movement treatment.
See Your Doctor Within 1 to 2 Weeks For:
- Leg pain or numbness that is not improving after 2 weeks of consistent self-management
- Symptoms that are getting progressively worse rather than better
- Weakness in one leg or foot — even mild weakness warrants assessment
- Your first-ever significant sciatica episode — to rule out serious underlying causes and get a confirmed diagnosis
- Pain severe enough to be preventing sleep on most nights
When to See a Physiotherapist:
A physiotherapist can assess the specific cause of your sciatica (disc herniation, piriformis syndrome, or spinal stenosis), identify your specific movement dysfunctions, and create a targeted exercise and manual therapy programme. Consider booking an assessment if:
- Generic exercises are not providing improvement after 3 to 4 weeks
- Your symptoms keep recurring despite self-management efforts
- You are unsure which exercises are appropriate for your specific type of sciatica
People who sit for extended periods in jobs that involve driving or traveling should consider specialised seating solutions — coccyxrelief.com offers detailed guidance on coccyx and sciatic nerve pressure-relieving cushions for prolonged sitting, including vehicle-specific options.
Frequently Asked Questions
How long can I sit before sciatica flares up?
Most people with active sciatica symptoms should limit unbroken sitting to 30 to 45 minutes. Research shows lumbar disc pressure increases by 40 to 90% in a seated position compared to standing, and this mechanical load accumulates progressively over time. If you have a herniated disc or prior sciatica episodes, even 20 minutes of unbroken sitting may provoke symptoms. Set a timer and stand up to move briefly at least every 30 minutes — this simple habit is one of the most effective preventive strategies available.
What is the best sitting position for sciatica?
The best sitting position for sciatica maintains the natural inward curve of the lumbar spine. Sit with your feet flat on the floor, knees at 90 degrees, hips at or slightly above knee height, and use a lumbar support cushion placed at the small of your back. Avoid slouching, crossing your legs, or sitting with a wallet in your back pocket. An ergonomic chair with adjustable lumbar support and seat height provides the foundation for this posture. For extended sitting, alternate between sitting and standing every 30 to 45 minutes.
Does sitting too long cause permanent sciatica?
Sitting too long does not directly cause permanent sciatica, but it accelerates the disc degeneration and spinal changes that can lead to chronic nerve compression. Most sitting-triggered sciatica episodes resolve within 4 to 12 weeks with appropriate management. However, repeated unmanaged flare-ups combined with inactivity, excess weight, and poor posture can create a cycle of progressive disc deterioration that increases the risk of recurrent or chronic sciatica. Consistent prevention — regular movement, core strengthening, and good posture — is the best protection.
What should I do immediately when sciatica flares up from sitting?
Stand up immediately and walk for 5 minutes at a gentle pace. Then perform 10 McKenzie press-ups (lie face down, push upper body up keeping hips on the floor, hold 5 seconds each). Follow with a piriformis stretch: lie on your back, cross the affected ankle over the opposite knee, and pull the bottom leg toward your chest for 30 seconds each side. Apply heat to the lower back and buttock for 10 to 15 minutes. Avoid sitting back down until the sharp pain has eased. If pain is severe or accompanied by leg weakness, contact your healthcare provider.
Can an ergonomic chair prevent sciatica from sitting?
An ergonomic chair significantly reduces the risk of sitting-triggered sciatica by supporting proper lumbar lordosis and distributing body weight more evenly. However, no chair alone prevents sciatica. Even the best ergonomic chair requires correct posture, regular movement breaks every 30 to 45 minutes, and daily stretching and core strengthening. The chair is one component of a broader prevention strategy. A good ergonomic chair combined with a sit-stand desk and regular movement breaks is more effective than any single intervention on its own.
Why does sciatic nerve pain get worse when sitting at a desk?
Desk sitting worsens sciatica through several compounding mechanisms. Sitting increases lumbar disc pressure by 40 to 90% compared to standing, pushing disc material toward the sciatic nerve root. Without lumbar support, the lower back rounds and flattens the natural curve, increasing disc strain further. The piriformis muscle shortens and tightens from sustained hip flexion, potentially squeezing the sciatic nerve in the buttock. Leaning toward a screen shifts the centre of mass forward, multiplying stress at the L4-L5 and L5-S1 levels where most sciatica originates. All of these factors worsen progressively across the working day if not actively counteracted.
Sources & Methodology
This article was written using current clinical evidence, peer-reviewed biomechanics research, and the professional experience of Dr. Sarah Mitchell, a licensed physical therapist with more than 12 years of clinical experience specialising in sciatica and lumbar radiculopathy. All exercise and posture recommendations are drawn from established clinical guidelines and primary research.
Primary Sources:
-
Nachemson, A.L. (1981). "Disc pressure measurements." Spine, 6(1), 93–97. Foundational research measuring intradiscal pressure in living subjects across postures, including the seminal seated posture data cited throughout this article.
-
Wilke, H.J., Neef, P., Caimi, M., Hoogland, T., & Claes, L.E. (1999). "New in vivo measurements of pressures in the intervertebral disc in daily life." Spine, 24(8), 755–762. Updated in vivo disc pressure measurements confirming Nachemson's findings with improved methodology.
-
McGill, S.M. (2015). Low Back Disorders: Evidence-Based Prevention and Rehabilitation (3rd edition). Human Kinetics. Dr. McGill's foundational text on spinal biomechanics and the core stabilisation exercises (bird-dog, modified plank) recommended in this article.
-
McKenzie, R., & May, S. (2003). The Lumbar Spine: Mechanical Diagnosis and Therapy (2nd edition). Spinal Publications. The clinical basis for the McKenzie press-up and standing extension techniques recommended for immediate relief.
-
Deyo, R.A., Diehl, A.K., & Rosenthal, M. (1986). "How many days of bed rest for acute low back pain?" New England Journal of Medicine, 315(17), 1064–1070. Landmark study demonstrating that activity outperforms bed rest for lumbar radiculopathy — the evidence base for recommending walking and movement over rest.
-
National Institute for Health and Care Excellence (NICE). (2020). "Low back pain and sciatica in over 16s: assessment and management." NICE guideline NG59. Current UK clinical practice guidelines informing assessment and red flag criteria used in this article.
-
Shiri, R., & Falah-Hassani, K. (2016). "The effect of smoking on the risk of sciatica: a meta-analysis." The American Journal of Medicine, 129(1), 64–73. Quantified the risk increase for lumbar radiculopathy in smokers.
Methodology: Exercise recommendations were selected based on three criteria: (1) support from peer-reviewed research or systematic review, (2) appropriateness for home use after initial instruction, and (3) targeting at least one of the four mechanisms by which sitting triggers sciatica: disc pressure, piriformis compression, hip flexor tightening, and nerve sensitisation. Red flag criteria are based on NICE NG59 guidelines and standard physiotherapy clinical practice.
This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before beginning any new exercise programme, especially if your sciatica is severe, has not been formally assessed, or is accompanied by leg weakness, bowel or bladder changes, or saddle area numbness.
About the Author: Dr. Sarah Mitchell is a licensed physical therapist specialising in musculoskeletal pain and spinal rehabilitation with over 12 years of clinical experience treating sciatica and lumbar radiculopathy. She holds a Doctor of Physiotherapy from the University of Melbourne and is a member of the Australian Physiotherapy Association. Dr. Mitchell writes for SciaticaSpot to help patients understand and manage their sciatic nerve pain with evidence-based, practical guidance.