Condition Guides
Sciatica vs Piriformis Syndrome: Key Differences
Sciatica vs piriformis syndrome: how to tell the difference, diagnostic tests, pain patterns, and which treatment works for each condition. Expert guide 2026.
📽️ 30-Second Summary
Sciatica vs Piriformis Syndrome
They feel the same — but the treatment is completely different
Disclosure: Sciatica Spot may earn a commission from qualifying purchases. This does not influence our recommendations.
By Dr. Rachel Thompson, Physical Therapist · Last updated March 2026
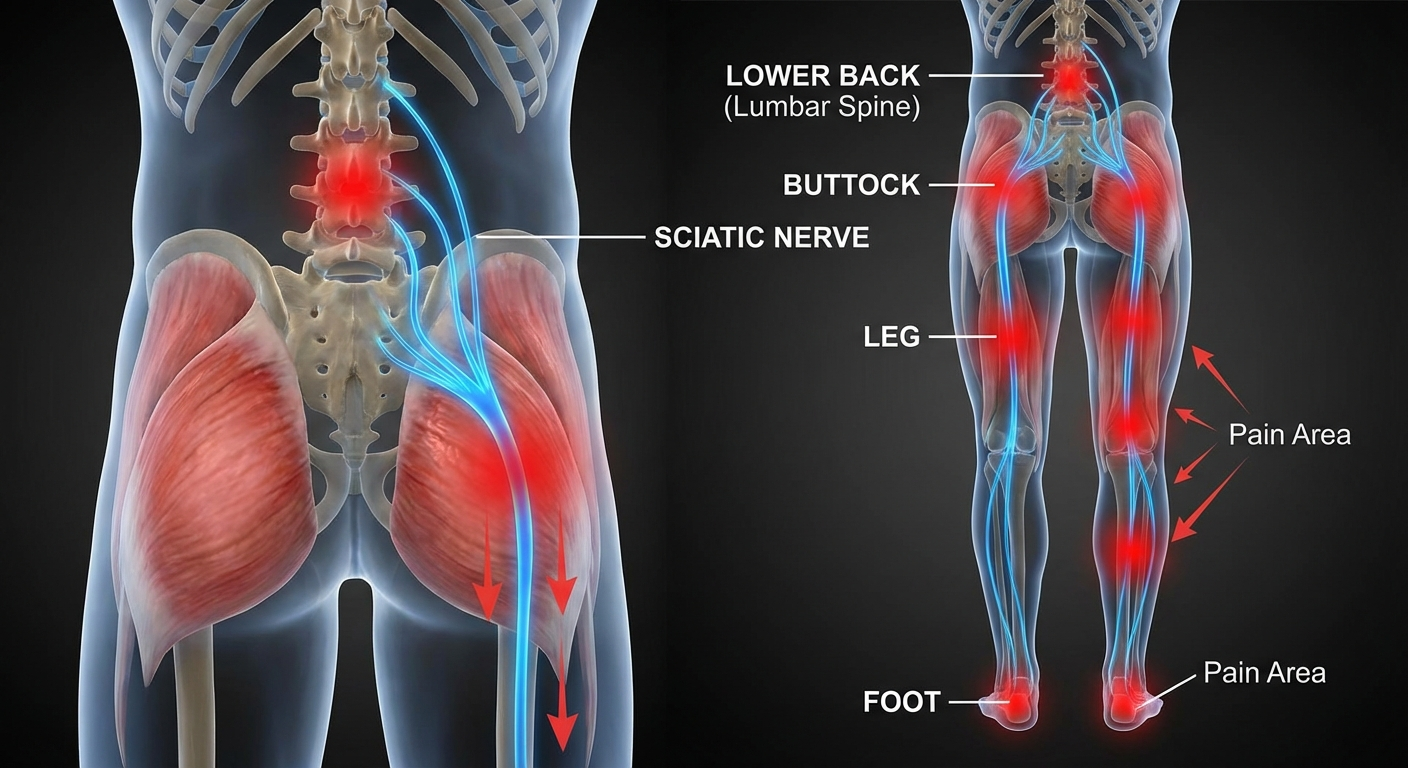
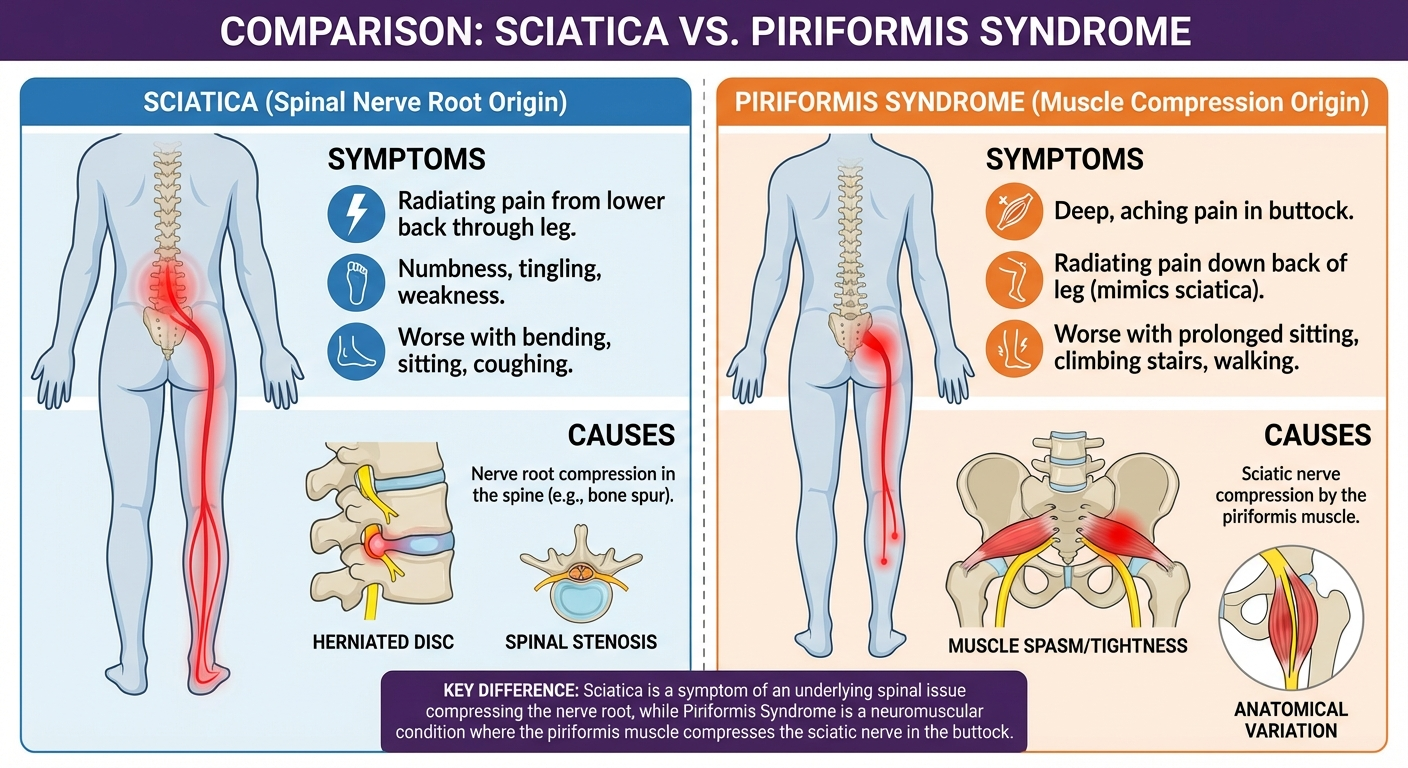
Sciatica and piriformis syndrome cause nearly identical symptoms — pain and tingling radiating from the buttock down the leg — but have completely different causes. Sciatica originates at the spine from a herniated disc or bone spur compressing the sciatic nerve root. Piriformis syndrome originates in the buttock, where the piriformis muscle compresses the sciatic nerve as it passes through or under the muscle. Treatment is fundamentally different for each. Misdiagnosis leads to months of ineffective treatment.
Quick Comparison: Sciatica vs Piriformis Syndrome
| Feature | Sciatica (Disc/Spinal) | Piriformis Syndrome |
|---|---|---|
| Origin of compression | Spine (disc, bone spur, stenosis) | Piriformis muscle in buttock |
| MRI findings | Disc herniation, stenosis visible | Usually normal |
| Pain location | Lower back + buttock + leg | Buttock (deep) + leg, often minimal back pain |
| Worse with | Sitting, bending forward | Sitting, hip rotation, crossing legs |
| Better with | Walking, lying flat | Walking, changing positions |
| FAIR test | Usually negative | Usually positive |
| Straight leg raise | Often positive | Less commonly positive |
| Treatment | McKenzie method, nerve glides, possibly surgery | Piriformis stretching, PT, massage |
What is Sciatica?
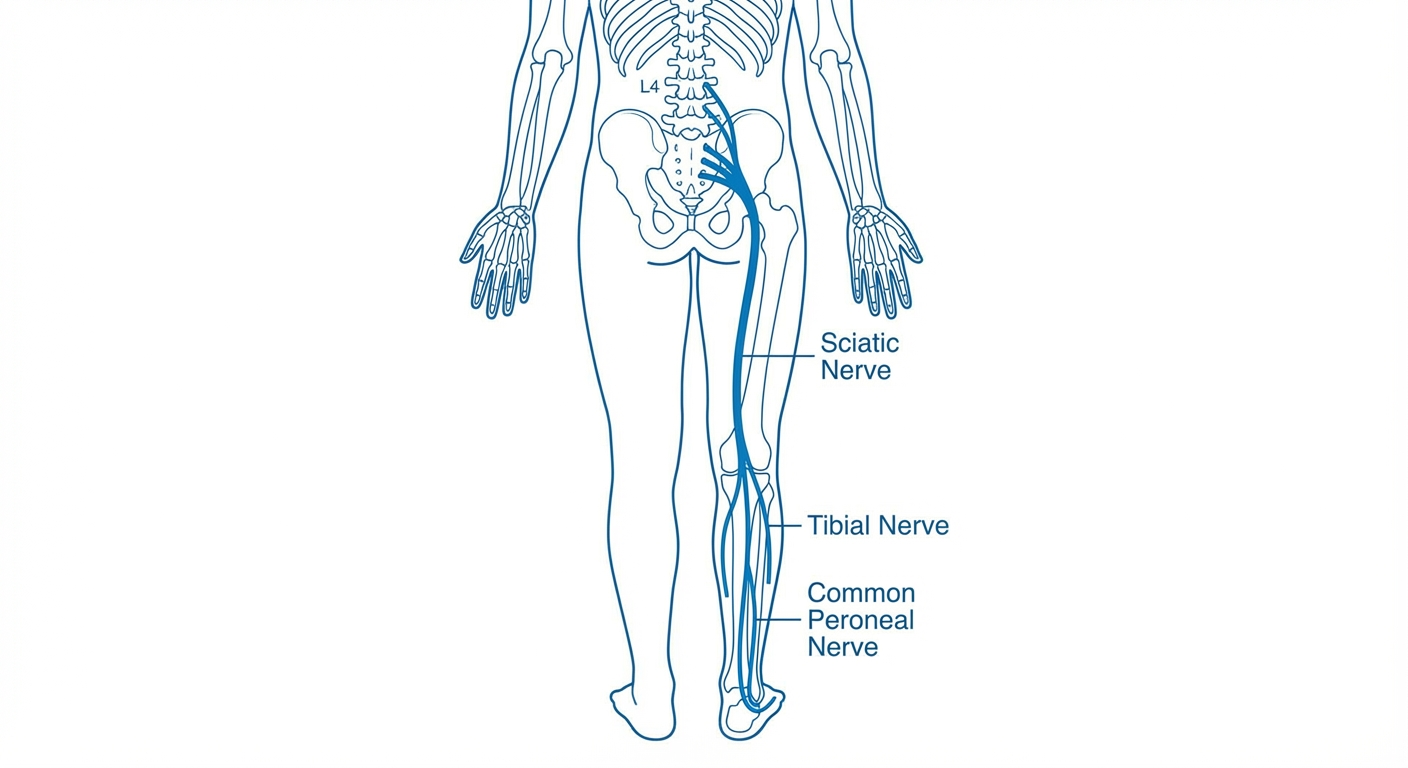
Sciatica is not a diagnosis — it is a symptom. It describes pain that radiates along the path of the sciatic nerve, which runs from your lower back through your buttocks and down each leg. For a deeper look at how long episodes typically last and what affects recovery time, see our guide on how long does sciatica last.
Causes of True Sciatica
The most common cause is disc herniation — when the soft center of a spinal disc pushes through the outer ring and presses on a nerve root.
| Cause | Mechanism | Common Level |
|---|---|---|
| Disc herniation | Disc material compresses nerve root | L4–L5, L5–S1 |
| Bone spur (osteophyte) | Bony growth narrows the spinal canal | L3–L4, L4–L5 |
| Spinal stenosis | Canal narrows from degenerative changes | L3–L4, L4–L5 |
| Spondylolisthesis | Vertebra slips forward, pinching nerve | L4–L5 |
| Pregnancy | Fetal position compresses sciatic nerve | Variable |
Pregnancy-related sciatica deserves its own discussion — the causes, timeline, and safe treatment options differ significantly from disc-related sciatica. Our guide on sciatica during pregnancy covers these differences in detail.
Classic Sciatica Symptoms
- Lower back pain (usually present, can be severe)
- Buttock pain radiating into the leg
- Pain follows a dermatomal pattern (specific nerve root path)
- Worsens with sitting, especially leaning forward
- Worsens with coughing, sneezing, or straining (increases disc pressure)
- May improve with walking (reduces disc pressure compared to sitting)
- Tingling or numbness in the leg or foot
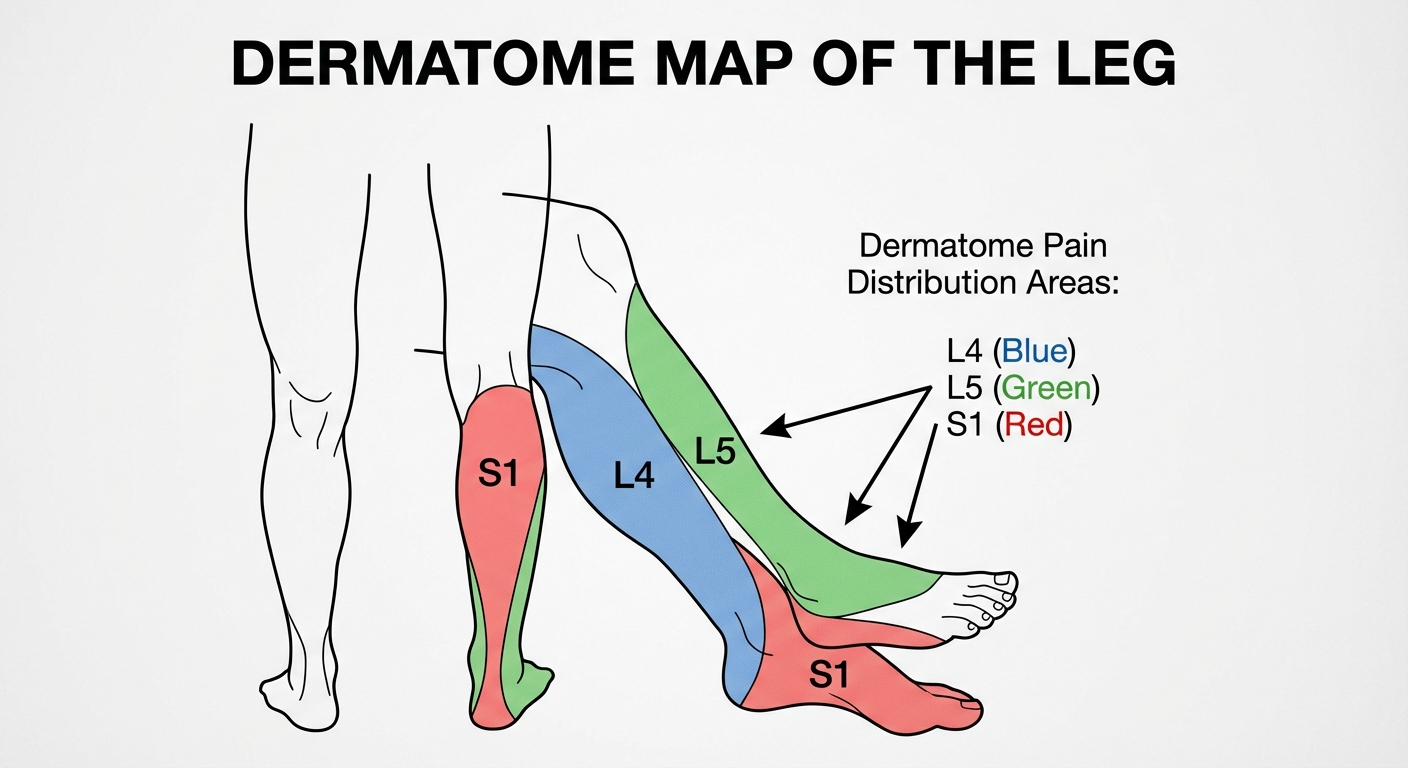
L4–L5 vs L5–S1 Sciatica
The level of nerve compression affects where symptoms appear:
| Level | Pain Pattern | Weakness | Reflex Affected |
|---|---|---|---|
| L4 root | Inner shin to foot | Foot dorsiflexion | Knee reflex |
| L5 root | Outside calf to top of foot | Big toe extension | None commonly |
| S1 root | Back of calf to little toe | Calf raise | Ankle reflex |
What is Piriformis Syndrome?
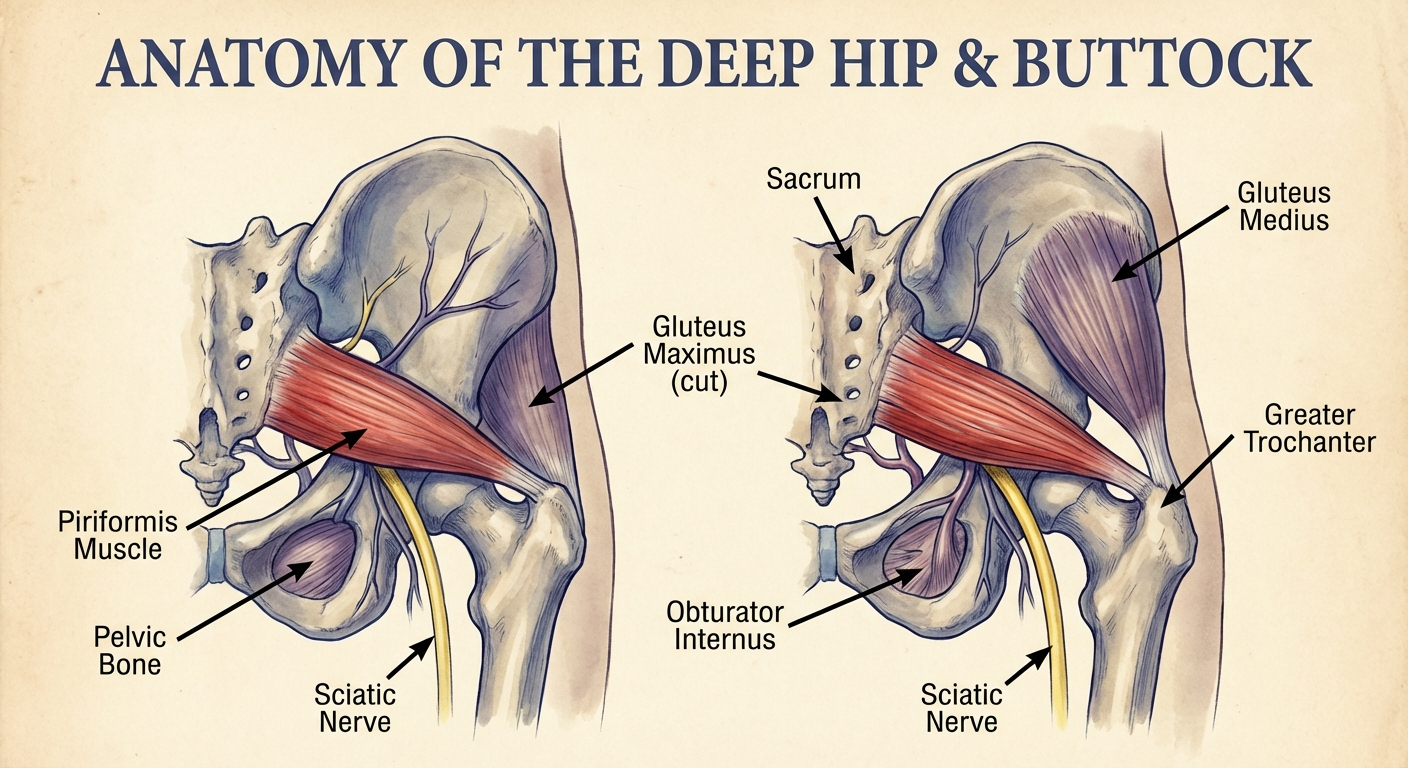
Piriformis syndrome occurs when the piriformis muscle — a small, deep muscle in the buttock that externally rotates the hip — compresses or irritates the sciatic nerve as it passes nearby.
Anatomy of the Problem
In approximately 83% of people, the sciatic nerve passes below the piriformis muscle. In approximately 17%, the nerve passes through the muscle itself. This anatomical variation makes some people more susceptible to piriformis syndrome.
When the piriformis becomes tight (from prolonged sitting, overuse, trauma, or muscle imbalance), it can compress the adjacent sciatic nerve, causing symptoms that mimic disc-related sciatica.
Causes of Piriformis Syndrome
| Cause | Who It Affects |
|---|---|
| Prolonged sitting | Office workers, drivers, students |
| Direct trauma to buttock | Falls, sports impacts |
| Overuse in running or cycling | Runners, cyclists, triathletes |
| Hip muscle imbalance (weak glutes) | Common in sedentary adults |
| Leg length discrepancy | Creates compensatory piriformis tension |
| Postpartum changes | Altered pelvic mechanics |
Classic Piriformis Syndrome Symptoms
- Deep buttock pain — specifically in the center of the buttock
- Leg pain follows the sciatic nerve path but may be less consistent than disc sciatica
- Minimal or no lower back pain — key distinguishing feature
- Worsens with sitting (especially with one leg crossed over the other)
- Worsens with hip internal rotation (e.g., turning toes inward)
- Point tenderness in the buttock on direct palpation
- Pain with prolonged walking or climbing stairs
How to Tell the Difference
The Two Most Useful Self-Tests
Test 1: Back Pain Test
Does your pain include significant lower back pain?
- Yes, lower back pain present → More likely true sciatica (spinal cause)
- No, mainly buttock and leg pain, little or no back pain → More likely piriformis syndrome
Test 2: Sitting Position Test
When you sit with your legs uncrossed:
- Pain worsens within 5–10 minutes → Could be either
- Pain dramatically worsens when crossing the affected leg over the other → More likely piriformis syndrome (this position stretches and presses on the piriformis)
Test 3: Forward Bend Test
Stand and slowly bend forward to touch your toes:
- Pain shoots down the leg during forward bending → More likely disc sciatica (increased disc pressure on the nerve root)
- Forward bending does not increase leg pain → More likely piriformis syndrome

Diagnostic Tests
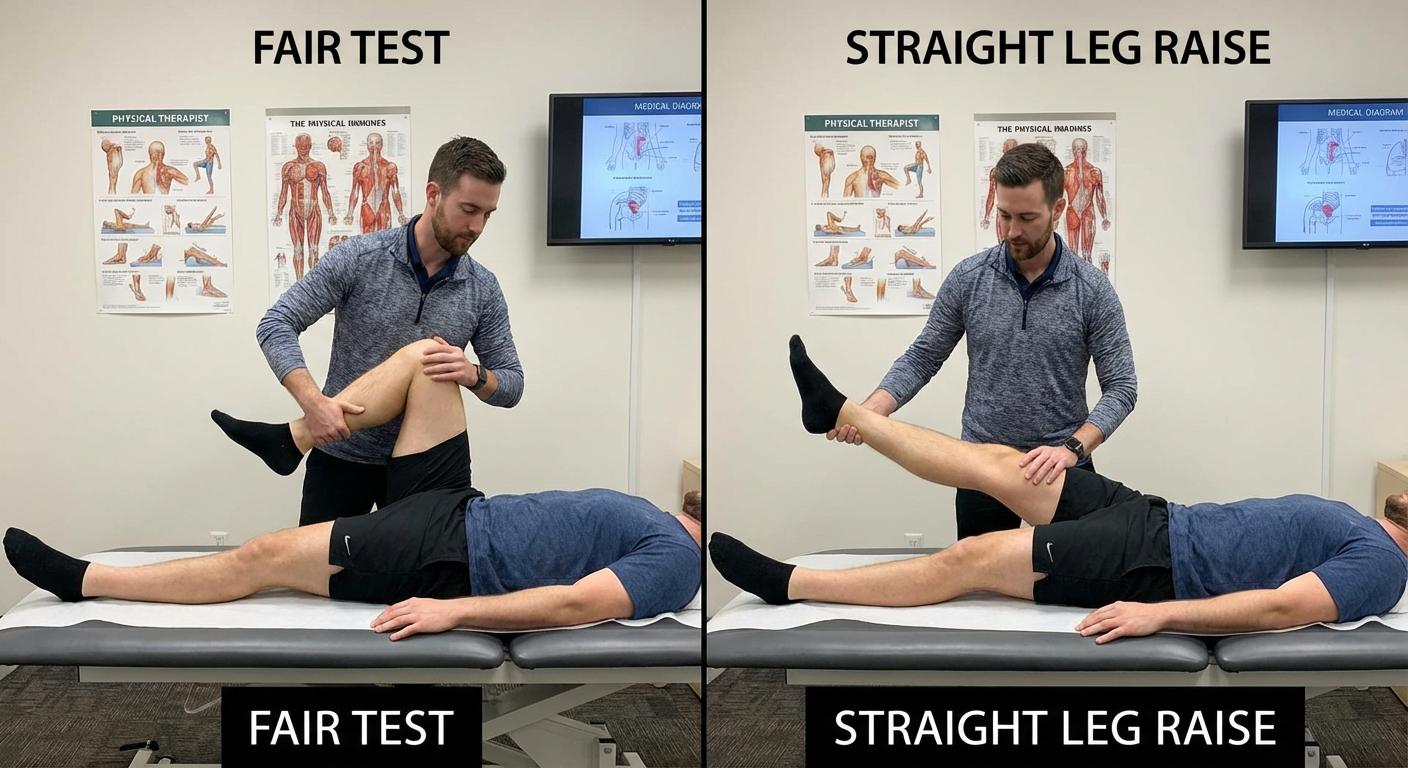
The FAIR Test (Piriformis-Specific)
The FAIR test (Flexion, Adduction, Internal Rotation) is the most clinically useful bedside test for piriformis syndrome:
Procedure:
- Lie on your back
- Flex the hip to 60° (bend the knee, lift the foot off the table)
- Adduct the hip (move the knee toward the centerline)
- Internally rotate the hip (turn the foot outward)
Result: If this position reproduces your buttock and leg pain within 30 seconds, the test is positive for piriformis syndrome. This position maximally stretches and loads the piriformis muscle.
Straight Leg Raise Test (Sciatica-Specific)
The straight leg raise (SLR) test is the classic test for disc-related sciatica:
Procedure:
- Lie flat on your back
- Have someone slowly lift your leg while keeping the knee straight
- The test is positive if leg pain radiates below the knee between 30–70° of elevation
Result: Positive SLR indicates sciatic nerve tension at the spine (from disc herniation). The SLR test is less commonly positive in piriformis syndrome because it doesn't stress the piriformis.
Imaging
| Test | Sciatica | Piriformis Syndrome |
|---|---|---|
| Standard MRI | Shows disc herniation, stenosis | Usually normal |
| MRI-neurography | Not typically helpful | May show nerve compression at piriformis |
| CT scan | Shows bony stenosis | Not helpful |
| X-ray | Shows bone changes, alignment | Not helpful |
| EMG/nerve conduction | May show nerve damage pattern | May help exclude spinal cause |
Pain Patterns Compared
Sciatica Pain Pattern
- Typically starts in the lower back or upper buttock
- Follows a consistent dermatomal path (outer calf for L5, back of calf for S1)
- May include numbness and tingling in a specific foot region
- Often a sharp, electric, shooting quality
- Usually on one side only
Piriformis Syndrome Pain Pattern
- Starts in the deep center of the buttock
- Pain may be less dermatomally consistent (sciatic compression outside the spine can affect the whole nerve)
- Tenderness in the piriformis region on direct pressure
- Sometimes a deep, aching quality in addition to radiating pain
- Often described as worsening with sitting more than any other position
Understanding exactly which activities trigger your symptoms is critical for diagnosis. Many of the same sciatica flare-up triggers — prolonged sitting, heavy lifting, sudden twisting — can also provoke piriformis syndrome, but the mechanism is different.
Sitting and Driving Pain
Both conditions worsen with prolonged sitting, but for different reasons:
Sciatica + sitting: Sitting increases lumbar disc pressure by 40–90% compared to standing. This increased pressure directly increases nerve root compression, intensifying pain.
Piriformis + sitting: Sitting shortens and potentially tightens the piriformis muscle. The seated position also places the sciatic nerve directly against the muscle with body weight pressing down, increasing mechanical compression.
Driving specifically: Driving is particularly provocative for both conditions. The reclined hip angle, vibration from the vehicle, and limited position changes create sustained compression.
For managing seated pain and reducing sciatica and piriformis compression during driving, see our guide on best car seat cushions for sciatica. For comprehensive coccyx and tailbone support that reduces piriformis tension, resources from coccyxrelief.com cover related seating solutions. If your work involves extended sitting at a desk, choosing the right office seating also matters — officechairguides.com offers detailed reviews of ergonomic chairs that support proper posture and reduce sciatic nerve compression.
Treatment: Sciatica
Phase 1: Acute Pain (First 1–4 Weeks)
- Relative rest (not bed rest — gentle movement is better than complete rest)
- Ice or heat for pain modulation (whichever provides relief — typically ice for first 48–72 hours, then heat)
- NSAIDs (ibuprofen, naproxen) for inflammation and pain
- Avoid positions that worsen pain (prolonged sitting, forward bending)
- Walking is generally beneficial — reduces disc pressure compared to sitting
Phase 2: Active Treatment (Weeks 2–12)
- McKenzie Method (extension exercises): Press-ups and sustained extension reduce disc material posteriorly, reducing nerve compression — first-line physical therapy for disc sciatica
- Nerve mobilization/neural flossing: Gentle sciatic nerve mobilization exercises
- Core stabilization: Strengthening deep abdominal and lumbar stabilizers to protect the disc
For a complete breakdown of which exercises help versus which exercises make disc sciatica worse, see our guide on sciatica exercises to avoid. Choosing the wrong exercise is one of the most common reasons people fail to improve.
Phase 3: Persistent or Severe Cases
- Epidural steroid injection: Corticosteroid delivered adjacent to the inflamed nerve root — effective short-term, evidence-limited long-term
- Surgery (microdiscectomy): For severe neurological deficit, loss of bladder/bowel control, or failure to improve after 6–12 weeks of conservative care
Treatment: Piriformis Syndrome
First-Line Treatment: Targeted Stretching
Piriformis syndrome responds more consistently to conservative treatment than disc sciatica. The primary treatment is stretching the piriformis muscle to reduce compression on the sciatic nerve.
Phase 1: Reduce Acute Inflammation
- Ice to the buttock (not lower back) 10–15 minutes, 2–3× daily
- NSAIDs for acute inflammation
- Reduce sitting time — standing and walking reduce piriformis tension
- Avoid activities that aggravate (running, cycling, stairs during acute phase)
Phase 2: Stretching and Physical Therapy
Three primary stretches:
1. Figure-Four Stretch (Supine)
- Lie on back, cross affected leg over the unaffected knee
- Grasp behind the unaffected thigh and pull toward chest
- Hold 30–60 seconds, 3× daily
2. Seated Piriformis Stretch
- Sit in chair, cross affected ankle over opposite knee
- Lean gently forward until stretch felt in buttock
- Hold 30 seconds, several times throughout the workday
3. FAIR Position Stretch
- Lie on back, use the FAIR test position as a therapeutic stretch
- Hold 30–60 seconds on each side, 2× daily

Phase 3: Advanced Treatments
- Trigger point massage/dry needling: Releases piriformis trigger points — often highly effective
- Corticosteroid injection into piriformis: Can provide extended relief
- Botulinum toxin injection: Reserved for refractory cases — relaxes the muscle for 3–6 months
- Surgical piriformis release: Rarely needed; considered only after extensive conservative treatment
Stretches and Exercises
For Piriformis Syndrome (These May Aggravate Disc Sciatica)
| Exercise | How to Do It | Sets × Duration |
|---|---|---|
| Figure-four stretch | Lying on back, ankle over knee, pull unaffected leg to chest | 3 × 30–60 sec |
| Seated piriformis stretch | Sitting, ankle over knee, lean forward | 3 × 30 sec, multiple times daily |
| FAIR stretch | Lying, hip flexed + adducted + internally rotated | 3 × 30 sec |
| Clamshell (glute med.) | Side-lying, feet together, open knees like clamshell | 3 × 15 reps |
For Disc Sciatica (These May Not Help Piriformis)
| Exercise | How to Do It | Sets × Duration |
|---|---|---|
| Prone press-up (McKenzie) | Lying face-down, push upper body up with arms, hips stay down | 10 × 10 sec holds |
| Standing extension | Hands on lower back, arch backward gently | 10 × 10 sec holds |
| Neural flossing | Seated, extend knee while pointing foot up, then down | 10 × each direction |

For a broader library of exercises with detailed progressions, see our full guide on sciatica exercises.
Recovery Timeline
Understanding realistic recovery timelines helps set expectations and prevents premature discouragement.
Sciatica Recovery Timeline
| Phase | Timeframe | What to Expect |
|---|---|---|
| Acute pain | Weeks 1–4 | Worst pain period; focus on pain management and avoiding aggravation |
| Active rehab | Weeks 4–12 | Gradual improvement with McKenzie and stabilization exercises |
| Resolution | 3–6 months | 80–90% of disc sciatica resolves with conservative treatment |
| Surgical cases | 6–12 months | Full recovery from microdiscectomy if conservative care fails |
Piriformis Syndrome Recovery Timeline
| Phase | Timeframe | What to Expect |
|---|---|---|
| Acute relief | Weeks 1–2 | Noticeable improvement with consistent stretching and ice |
| Significant improvement | Weeks 2–6 | Most patients see major reduction in symptoms |
| Full recovery | 6–12 weeks | Complete resolution with consistent physical therapy |
| Chronic cases | 3–6 months | May require injections or advanced intervention |
Key difference: Piriformis syndrome generally resolves faster with targeted treatment. Disc sciatica has a longer natural history because disc healing and nerve root inflammation take more time. However, piriformis syndrome has a higher recurrence rate if the underlying cause (weak glutes, prolonged sitting, poor posture) is not addressed long-term.
Sleep position also plays a significant role in recovery for both conditions. Lying in a position that maintains piriformis tension or increases disc pressure overnight can slow healing. Our guide on best sleeping positions for sciatica covers specific positioning strategies for each condition.
Product Recommendations
Ergonomic Seat Cushion
Reduces direct pressure on the piriformis region during prolonged sitting
View on AmazonFoam Roller for Piriformis
Self-myofascial release of the piriformis and surrounding hip muscles
View on AmazonLumbar Support for Sciatica
Maintains lumbar curve to reduce disc pressure and sciatic nerve root compression while seated
View on AmazonWhen to See a Doctor
See a doctor or emergency department immediately for:
- Loss of bladder or bowel control — this is cauda equina syndrome, a surgical emergency
- Progressive weakness in the leg — foot drop, inability to bear weight
- Severe pain uncontrolled by OTC medications
- Symptoms following a traumatic injury (fall, car accident)
- Bilateral symptoms (both legs affected)
See a doctor for evaluation within 1–2 weeks for:
- Leg pain not improving after 3–5 days of self-care
- First episode of significant sciatic pain (to rule out serious causes)
- Suspected piriformis syndrome not responding to stretching
Frequently Asked Questions
What is the difference between sciatica and piriformis syndrome?
Sciatica is caused by nerve compression at the spine. Piriformis syndrome is caused by the piriformis muscle in the buttock compressing the sciatic nerve. Both cause radiating leg pain, but the source and treatment differ fundamentally.
How do I know if I have sciatica or piriformis syndrome?
Key differentiators: sciatica worsens with forward bending and coughing; piriformis syndrome worsens with hip rotation and crossing legs. The FAIR test is positive in piriformis syndrome. MRI shows disc pathology in sciatica but is usually normal in piriformis syndrome.
Can you have both at the same time?
Yes — this is called double crush syndrome. The nerve can be compressed both at the spine and by the piriformis. Both sources require treatment.
Does piriformis syndrome show on MRI?
Standard MRI is usually normal. Diagnosis is primarily clinical based on the FAIR test and symptom pattern.
How do you treat piriformis syndrome?
Primary treatment: piriformis stretching (figure-four, FAIR stretch), physical therapy, and reducing prolonged sitting. For persistent cases: trigger point massage, corticosteroid injection, or botulinum toxin injection.
Is piriformis syndrome worse than sciatica?
Neither is universally worse. Piriformis syndrome often responds well to targeted stretching. Disc-related sciatica may require surgery in severe cases.
What exercises help piriformis syndrome but not sciatica?
Piriformis-specific stretches (figure-four, FAIR stretch, seated cross-leg stretch) directly target the piriformis muscle and are beneficial for piriformis syndrome. These same stretches may aggravate disc-related sciatica if they increase nerve tension. For disc-related sciatica, extension exercises (prone press-ups, McKenzie method) are often first-line; these are not specifically helpful for piriformis syndrome.
Sources and Methodology
Medical References:
- Boyajian-O'Neill LA, et al. "Diagnosis and Management of Piriformis Syndrome." Journal of the American Osteopathic Association, 2008.
- NICE guidelines: Low back pain and sciatica in adults — management — nice.org.uk
- Hopayian K, et al. "The clinical features of the piriformis syndrome: a systematic review." European Spine Journal, 2010.
- Fishman LM, et al. "Piriformis syndrome: Diagnosis, treatment, and outcome." Spine, 2002.
- McKenzie Institute International: MDT approach to mechanical spine pain
Product Note: This article provides educational information, not medical advice. Consult a healthcare professional for diagnosis and treatment of sciatica or piriformis syndrome.
By Dr. Rachel Thompson, Physical Therapist
Dr. Rachel Thompson is a licensed physical therapist specializing in musculoskeletal pain and spinal rehabilitation. This site may earn commissions from qualifying purchases. Last updated March 2026.